






Idiomas
Páginas
Jurídico

Aspectos generales del Síndrome X
Frágil
Dr. Josep ArtigasDra. Carme BrunDra. Elisabet Gabau
Hospital Parc TaulíSabadell
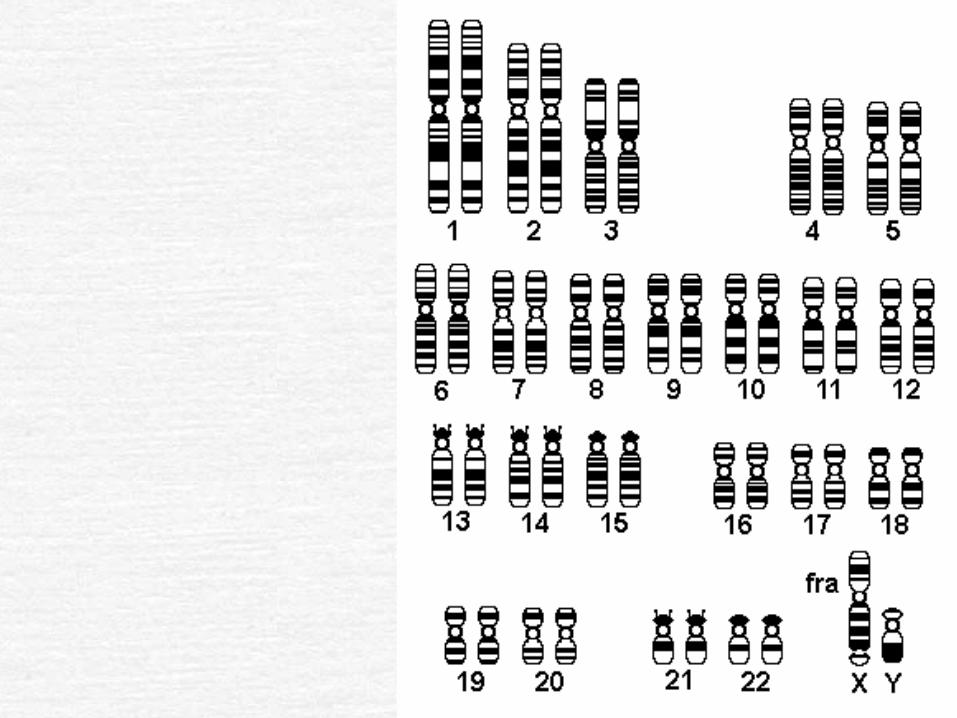
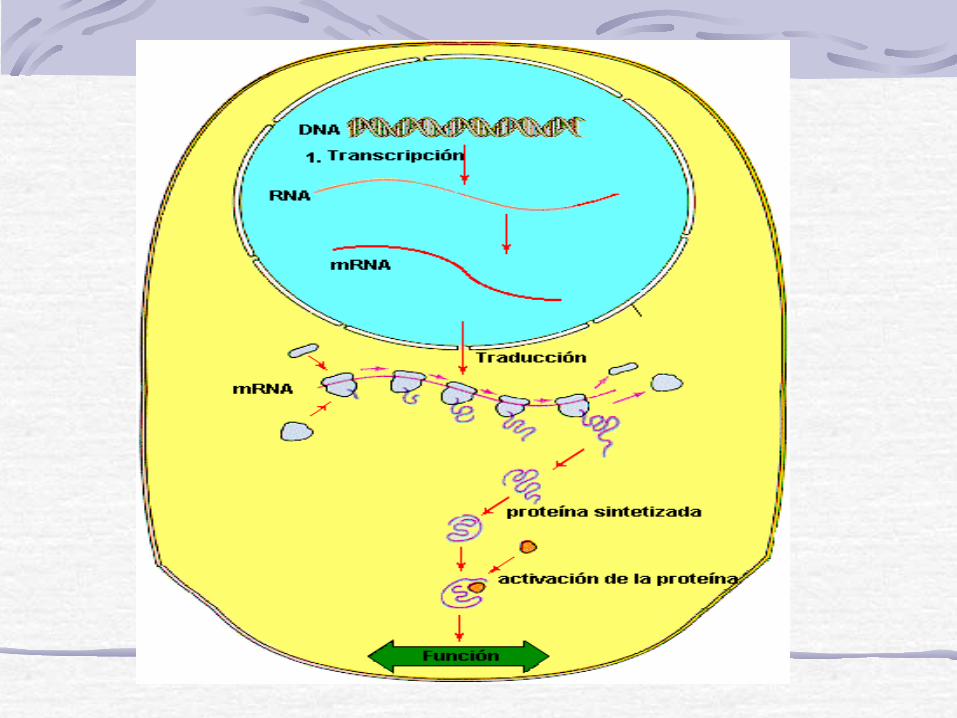
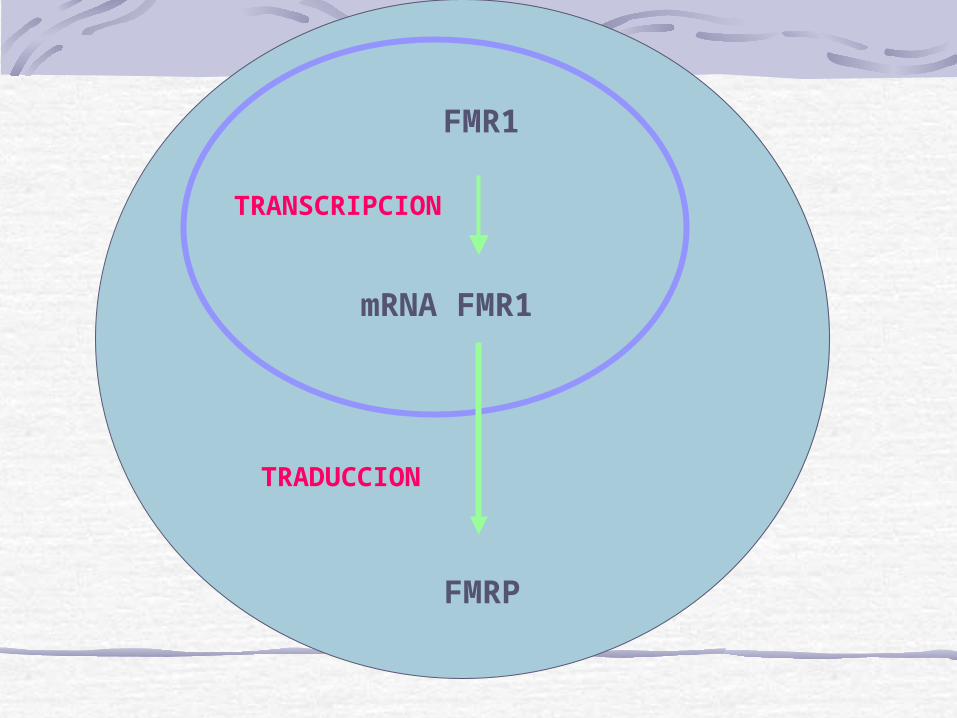
FMR1
mRNA FMR1
TRANSCRIPCION
FMRP
TRADUCCION
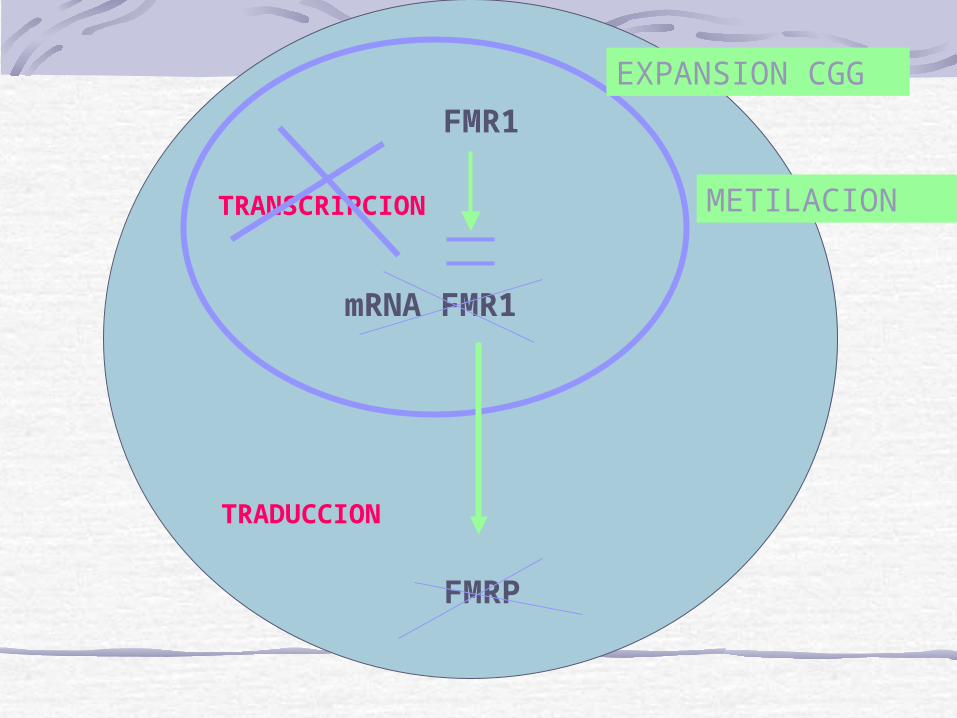
FMR1
mRNA FMR1
TRANSCRIPCION
FMRP
TRADUCCION
EXPANSION CGG
METILACION
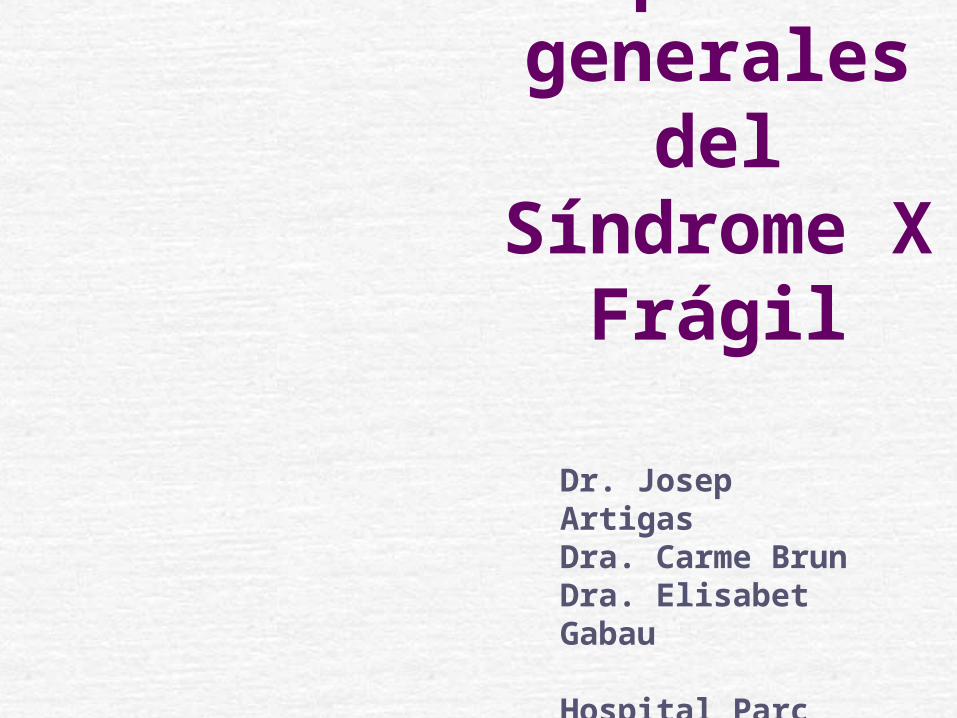
Fra X. Bases Genéticas (1)
Normal: 0-50 repeticionesPremutación: 50-200 repeticiones: no metilados y productores de proteína FMRPMutación completa: 200-2000 repeticiones: metilados y no productores de proteína FMRPLa metilación del gen evita la producción de proteína FMRP
Fra X. Bases Genéticas (2)La expansión a mutación completa solo sucede cuando una mujer premutada pasa la mutación a sus hijos/as.Cuando un hombre premutado pasa el Cr X a sus hijas no hay expansión.El hombre pasa la premutación a las hijas pero no a los hijos.

Fra X. Bases Genéticas (3)
Prevalencia de mujeres premutadas: 1/259Prevalencia de retardo mental y mutación completa:
hombres 1/ 4000mujeres 1/6000-8000
Características físicas. Faciales
(1)
Ausentes en el 25 - 30 %Cara alargadaOrejas prominentesMentón prominentePrognatismoEn mujeres se da el mismo fenotipo
Características físicas. Faciales (2)
Otras menos típicas
Fisuras palplebrales estrechasMacrocefaliaFrente prominenteEpicantusEstrabismoHipotoniaPaladar ojivalMaloclusión dental
METODOSCuestionarioPrincipales manifestaciones y conductas propias del síndromeEnviado a través de las Asociaciones Españolas de X Frágil

PACIENTESN. PACIENTES: 106 ( 95 niños, 11 niñas)EDAD MEDIA 12.79 (+/- 1.43)RANGO DE EDAD 2.3 - 43 EDAD DIAGNOSTICO 7.62 (+/-1.24)MUTACIONES:
3 premutación 62 mutación completa 1 mosaicismo40 desconocido

Edad de diagnóstico
0
5
10
15
20
25
< 77 78-80 81-83 84-86 87-89 90-92 93-95 96-98
Año del diagnóstico
Eda
d
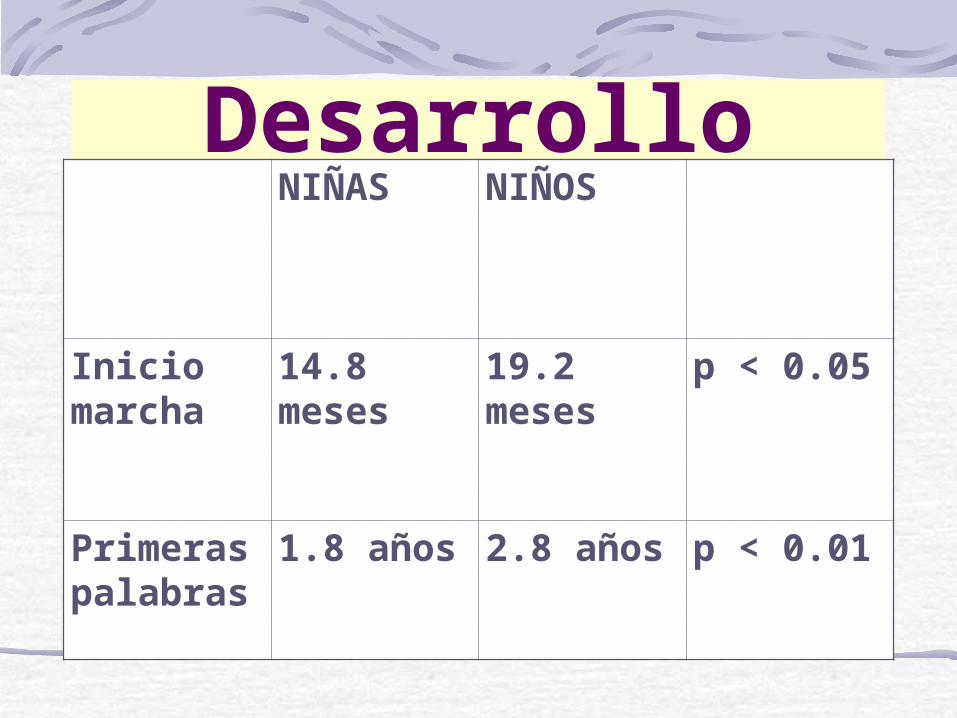
DesarrolloNIÑAS NIÑOS
Inicio marcha
14.8 meses
19.2 meses
p < 0.05
Primeras palabras
1.8 años 2.8 años p < 0.01

PROBLEMAS DE NARIZ Y OIDO
Algún problema crónico 54 %Otitis media recurrente 40 %Sinusitis recurrente 4 %Tubos timpánicos 17 %
Problemas oftalmológicos
Problemas oftalmológicos 43 %Estrabismo 25 %Problemas refractivos 21 %
Problemas ortopédicos
Problemas ortopédicos 58 %Pies planos 52 %Luxaciones articulares 9 %Luxación de cadera 5 %Hernias 7 %

Problemas cardiológicos
Prolapso mitralGeneralmente asintomáticoValoración cardiológica si se ausculta un soploProfilaxis de la endocarditis
Crecimiento y alteraciones
endocrinológicas
Crecimiento aumentado durante la infanciaDisfunción hipotalàmica. Sotos-likeFenotip Prader-Willi

MACROORQUIDISMO
80-95 % adolescentes-adultos> 30 mlempieza a partir de los 8-9 años
Problemas neurológicosHipotoníaApneas obstructivas del sueño 10 %Convulsiones 20 %Trastornos del sueño relacionados con la melatoninaProblemas cognitivosFenotipo conductual
Problemas del sueño
Insomnio14 %Roncar 45 %
Epilepsia
Convulsiones 14 %Edad media de la primera crisis 5.4 (+/- 2.1)Rango de edad de la primera crisis (0 – 14)Edad media de la última crisis 7,7 (+/- 2.8)Rango de edad de la última crisis 0.5 – 16
Fenotipo cognitivoMutación completa: QI: 41Mosaico: QI: 60Mutación completa/metilación parcial: QI: 8813 % de los niños no tienen retardo mentalK-ABC simultaneo>secuencialScore en aritmética (K-ABC) es el más bajo30 % presentan < QI a lo largo de los años, sin perder habilidades
FENOTIPO CONDUCTUAL
Conducta en sentido amplio (aspectos cognitivos e interacción social) asociada a un sindrome especifico con etiologia genética, en el cual no existe duda de que el fenotipo es resultado de la lesión subyacente

Fenotipo conductual (1)0 20 40 60 80 100
Problemas de atención
Aleteo de manos
Hiperactividad
Timidez
Agobiado por la muchedumbre
Ansiedad social
Agobiado por el ruido
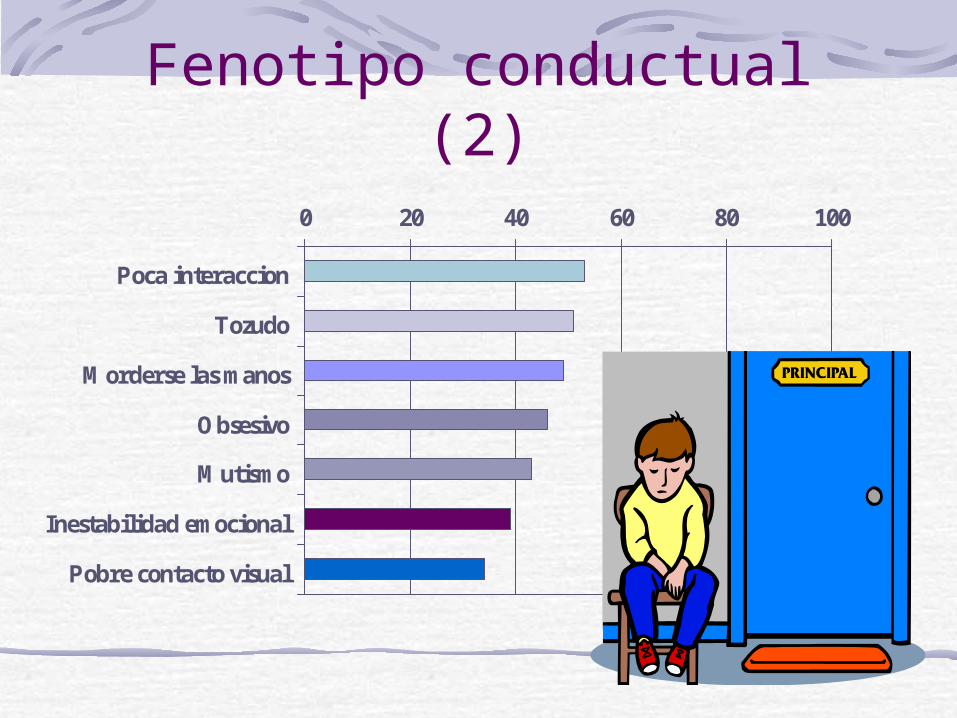
Fenotipo conductual (2)0 20 40 60 80 100
Poca interaccion
Tozudo
Morderse las manos
Obsesivo
Mutismo
Inestabilidad emocional
Pobre contacto visual
brun c, artigas j, gabau e
¿se puede explicar el fenotipo conductual del síndrome x-frágil por el retraso mental y por el trastorno de déficit de atención/hiperactividad?
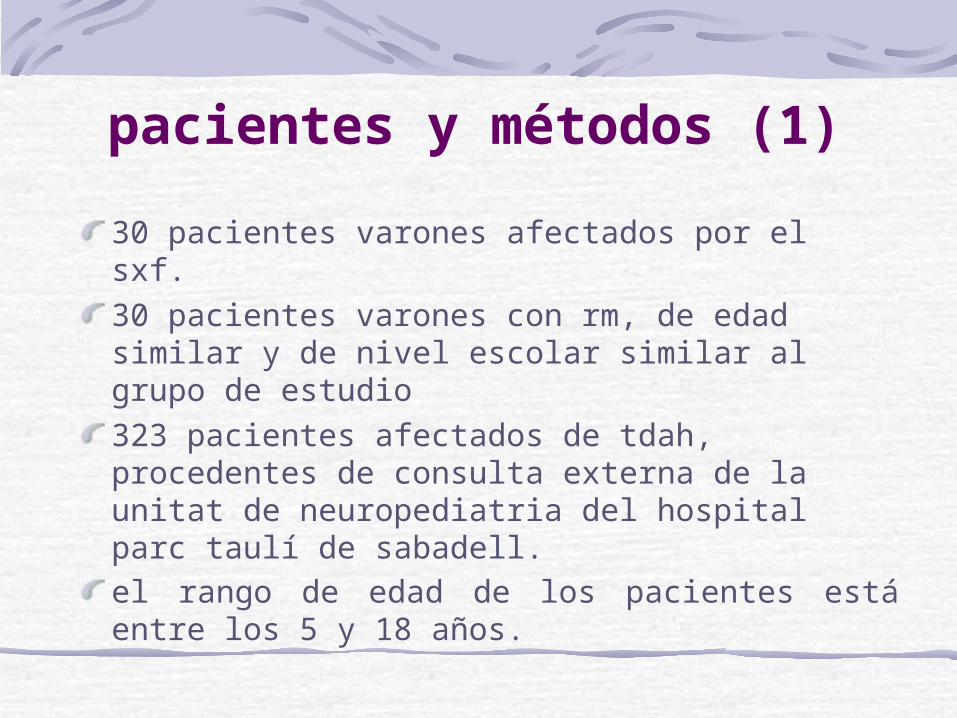
pacientes y métodos (1)
30 pacientes varones afectados por el sxf. 30 pacientes varones con rm, de edad similar y de nivel escolar similar al grupo de estudio323 pacientes afectados de tdah, procedentes de consulta externa de la unitat de neuropediatria del hospital parc taulí de sabadell.el rango de edad de los pacientes está entre los 5 y 18 años.
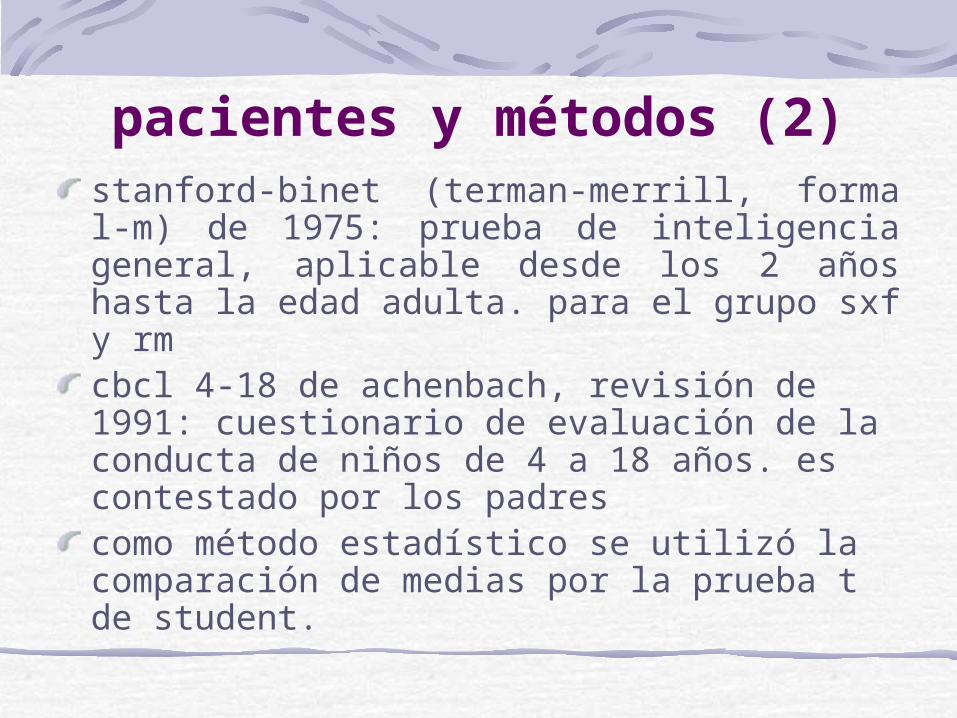
pacientes y métodos (2)stanford-binet (terman-merrill, forma l-m) de 1975: prueba de inteligencia general, aplicable desde los 2 años hasta la edad adulta. para el grupo sxf y rm cbcl 4-18 de achenbach, revisión de 1991: cuestionario de evaluación de la conducta de niños de 4 a 18 años. es contestado por los padres como método estadístico se utilizó la comparación de medias por la prueba t de student.
cbcl: cuestionario para padres, con 113 items sobre conductas concretas que permite valorar las siguientes escalas
aislamientoquejas somáticasansiedad/depresiónproblemas socialesproblemas de pensamiento
problemas de atenciónconducta delincuenteconducta agresivaescala internalizanteescala externalizanteescala total
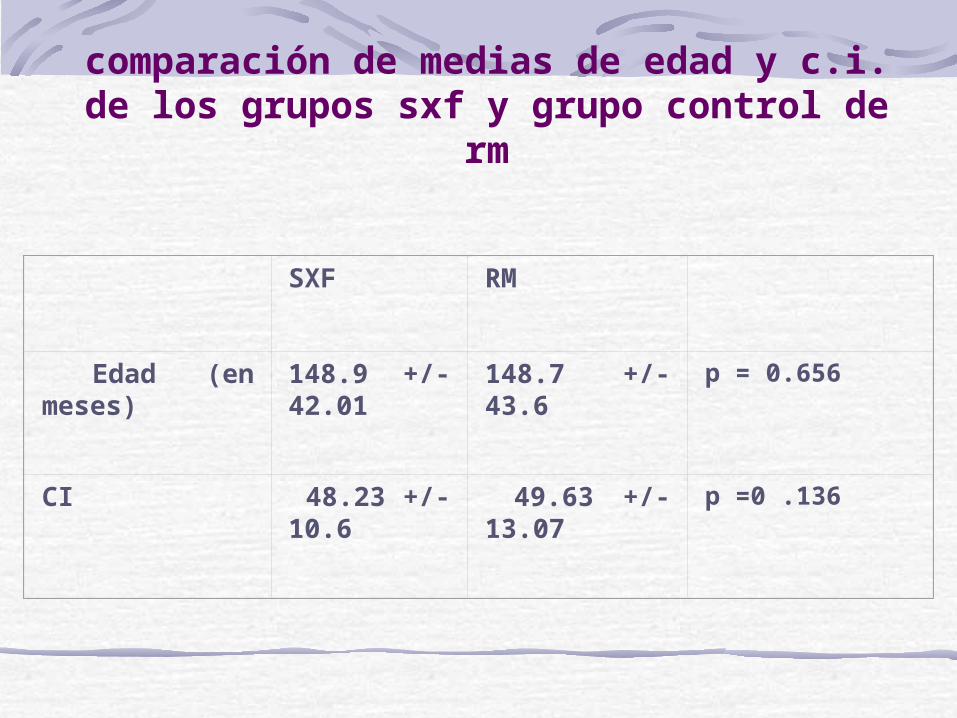
comparación de medias de edad y c.i. de los grupos sxf y grupo control de
rm
SXF RM
Edad (en meses) 148.9 +/-42.01 148.7 +/- 43.6 p = 0.656
CI 48.23 +/-10.6 49.63 +/- 13.07 p =0 .136
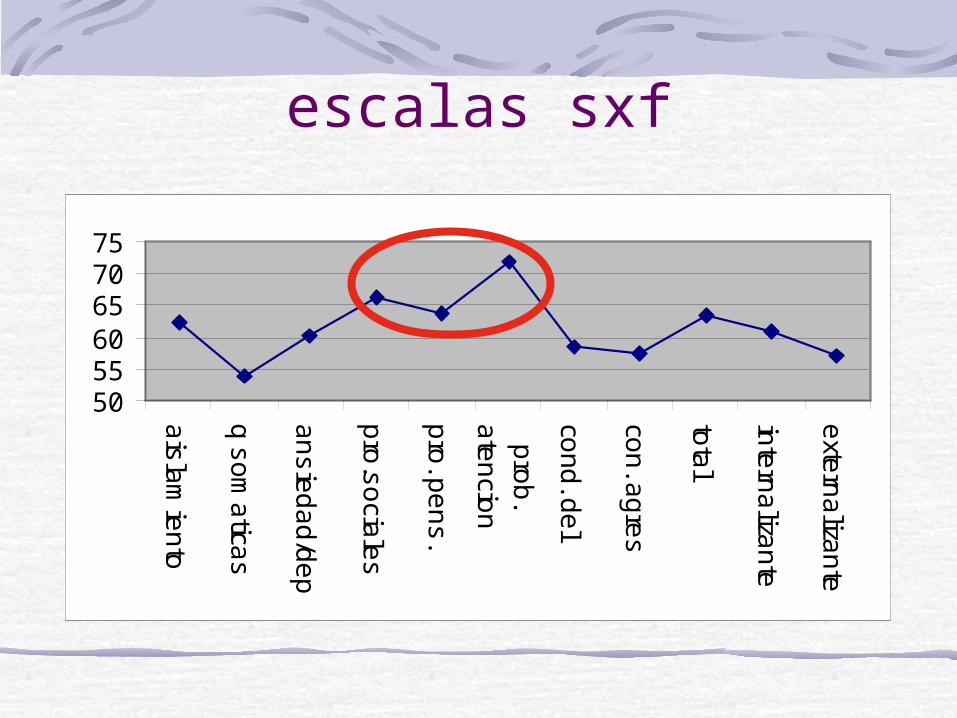
escalas sxf
505560657075
ais
lam
ien
to
q s
om
atica
s
an
sie
da
d/d
ep
pro
.so
ciale
s
pro
. pe
ns
.
pro
b.
ate
ncio
n
con
d. d
el
con
. ag
res
tota
l
inte
rna
lizan
te
exte
rna
lizan
te
características conductuales en niños con sxf valoradas con la cbcldb bailey. north carolina
59 niños (4 – 12 años)valoración anual51 % puntuaban significativamente en la escala totallas puntuaciones más altas aparecían en atención, pensamiento y problemas sociales
conductas más frecuentes en el grupo sxf (1)
no se puede concentrar o prestar atención por mucho ratonervioso, sensible o tensoactúa demasiado inmaduro para su edadvergonzosotímidoproblemas con la pronunciación o el hablano puede sentarse quieto, intranquilo, demasiado activotrabajo escolar deficiente apegado a los adultos, demasiado dependienterepite ciertos actos una y otra vezexige mucha atencióngestos nerviosos, tics
conductas más frecuentes en el grupo sxf (2)
se enfurruña o se incomoda fácilmenteimpulsivo, hace cosas sin pensarincordiando, torpejura, dice palabrotas rabietas, mal geniotiene miedo a ciertos animales, situaciones o lugares aparte de la escuelaasustadizo, ansioso
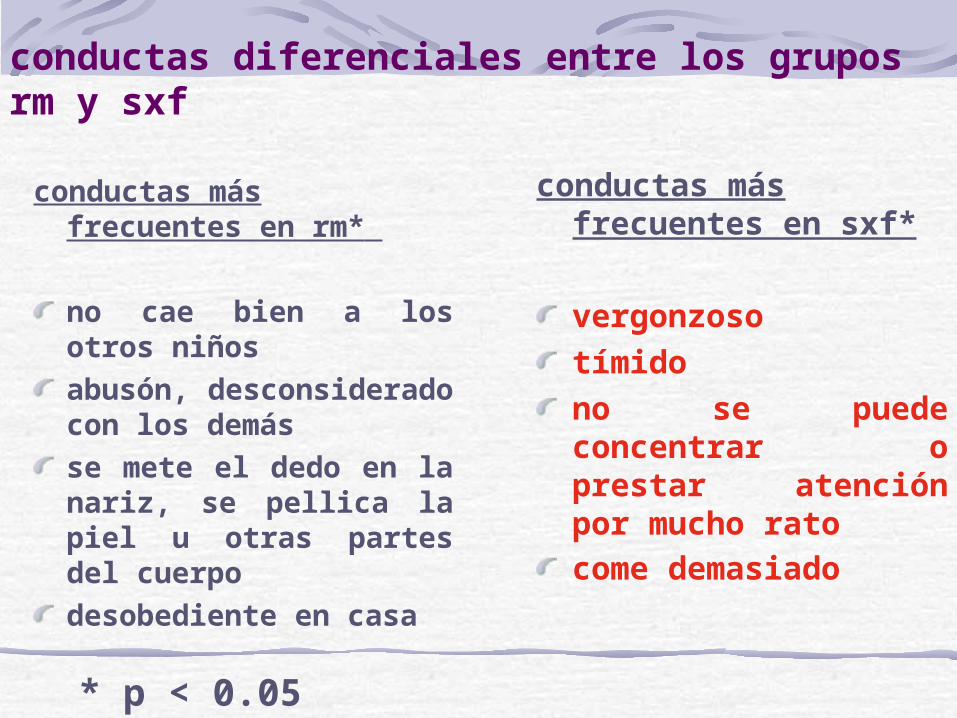
conductas diferenciales entre los grupos rm y sxf
conductas más frecuentes en rm*
no cae bien a los otros niñosabusón, desconsiderado con los demásse mete el dedo en la nariz, se pellica la piel u otras partes del cuerpodesobediente en casa
conductas más frecuentes en sxf*
vergonzosotímidono se puede concentrar o prestar atención por mucho ratocome demasiado
* p < 0.05
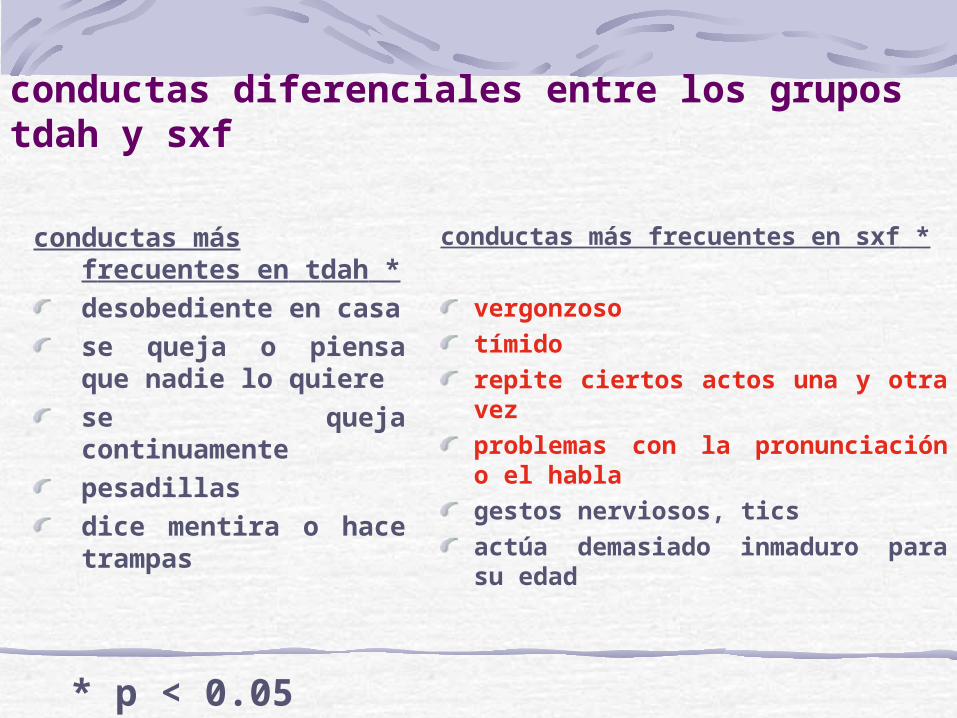
conductas diferenciales entre los grupos tdah y sxf
conductas más frecuentes en tdah *desobediente en casase queja o piensa que nadie lo quierese queja continuamentepesadillasdice mentira o hace trampas
conductas más frecuentes en sxf *
vergonzosotímidorepite ciertos actos una y otra vezproblemas con la pronunciación o el hablagestos nerviosos, ticsactúa demasiado inmaduro para su edad
* p < 0.05
Cortisol and social stressors in children with fragile X: a pilot study. Wisbeck JM. Huffman LC. Freund L. Gunnar MR. Davis EP. Reiss AL.Journal of Developmental & Behavioral Pediatrics. 21(4):278-82, 2000
en el sxf existe una disfunción neuroendocrinala conducta del sxf se caracteriza por ansiedad social y evitaciónalteraciones neuroanatómicas sugieren que la función hipotálamo-hiopofisaria-adrenal puede ser un componente del SXFlos SXF tienen niveles de cortisol superiores a la población normalniños/niñas sxf mismo nivel de cortisol basaldespués de un estresor social los niños más cortisol que las niñas
conclusionesLa escala CBCL detecta aspectos conductuales que no se explican por el RM o el TDAH que puede ir asociado al SXFlos aspectos relacionados con la ansiedad social (tímido, vergonzoso) destacan como aspectos diferenciales tanto con respecto al RM como al TDAHlas escalas de problemas de atención, problemas sociales y problemas de pensamiento, son las que muestran una puntuación más alta.

Aportaciones recientes al SXF

Screening for fragile X syndrome in women of reproductive age. Pesso R. Berkenstadt M. Cuckle H. Gak E. Peleg L. Frydman M. Barkai G.Prenatal Diagnosis. 20(8):611-4, 2000
9459 mujeres, 19 – 44 a. sin historia familiar de SXF134 portadoras; 1/70
130 premutación4 mutación completa
108 diagnósticos prenatales, 111 fetos9 mutación completa; 1/12
2 hijos de mutada completa7 expansiones
Prenatal diagnosis of fragile X syndrome and the risk of expansion of a premutation. Kallinen J. Heinonen S. Mannermaa A. Ryynanen M.Clinical Genetics. 58(2):111-5, 2000
60 – 80 repeticiones: 4.8 %. Si se transmite el alelo premutado: 14 %81 – 100 repeticiones: 61.5 %. Si se transmite el alelo premutado: 89 %40 – 59 repeticiones: Ninguna expansión
Cognitive and visual processing skills and their relationship to mutation size in full and premutation female fragile X carriers. Block SS. Brusca-Vega R. Pizzi WJ. Berry-Kravis E. Maino DM. Treitman TM.Optometry & Vision Science
• Woodcock-Johnson Psycho-Educational Battery-Revised, The Developmental Test of Visual Motor Integration, y cinco de los siete subtests del Test of Visual-Perceptual Skills
• Correlacion negativa, significativa entre la expansión y el rendimiento cognitivo

Monozygotic boys with fragile X syndrome. Sheldon L. Turk J. Developmental Medicine & Child Neurology. 42(11):768-74, 2000 Nov
a pesar de una constitucion genetica identica se observan diferencias en:
interaccion socialjuego simbolicolenguajevolumen del caudado
la anomalia del Xq27.3, no es suficiente para explicar el fenotipo conductual y la anatomia del SN
Fragile X males with unmethylated, full mutation trinucleotide repeat expansions have elevated levels of FMR1 messenger RNA. Tassone F. Hagerman RJ. Loesch DZ. Lachiewicz A. Taylor AK. Hagerman PJ.American Journal of Medical Genetics. 94(3):232-6, 2000 Sep 18
• La relación entre las repeticiones y la transcripción no ha sido establecida en el rango de mutación completa
• Previamente se demostró que el nivel de FMR1 mRNA esta elevado en la premutación
• los niveles de FMR1 mRNA permanecen elevados incluso para alelos que exceden 300 repeticiones
• Esta conclusión es independiente de la capacidad de transcripción en los alelos metilados
• La mutación completa, pero no es per se un impedimento para la transcripción.
Twin sisters, monozygotic with the fragile X mutation, but with a different phenotype. Willemsen R. Olmer R. De Diego Otero Y. Oostra BA.Journal of Medical Genetics. 37(8):603-4, 2000 Aug.
En dos hermanas monozgóticas con la mutación completa una era normal y la otra afectadaEn la hermana afectada solo una minoría de células tenían una expresión normal del FMR1Esto demuestra que la inactivación ocurre después de la separación del embrión
A majority of fragile X males with methylated, full mutation alleles have significant levels of FMR1 messenger RNA. Tassone F. Hagerman RJ. Taylor AK. Hagerman PJ. Journal of Medical Genetics, 38(7):453-6, 2001
FMR1 mRNA levels were determined in peripheral blood leucocytes for 48 fragile X males with methylated, full mutation alleles that are resistant to cleavage by methylation sensitive enzymes. Using quantitative (fluorescence) RT-PCR, we observed that more than half of these males produce FMR1 mRNA, with some mRNA levels approaching those found in normal subjects. In none of the samples analysed was there any evidence of premutation alleles. These results suggest that the assumed relationship between enzyme resistance and FMR1 gene silencing may not be generally valid. Despite the presence of FMR1 mRNA in some subjects, no FMRP production was detected by either immunocytochemistry or western blotting. The low/absent FMRP levels are probably a reflection of a post-trancriptional effect such as a defect in translation.
Bennetto L. Pennington BF. Porter D. Taylor AK. Hagerman RJ. Profile of cognitive functioning in women with the fragile X mutation. [Journal Article] Neuropsychology. 15(2):290-9, 2001 April.
Two studies tested the specificity of the neurocognitive profile of women with fragile X syndrome (FXS). First, women with an FXS full mutation were compared with women with a premutation and women without FXS who grew up in FXS families. Women with FXS had a significantly lower IQ than the other groups, and analyses of subtest profiles showed they had a relative weakness on Arithmetic and strength on Picture Completion. Women with FXS performed worse than the other groups on executive function, spatial ability, and visual memory. Next, women with FXS were compared with women without FXS matched on age and IQ. A similar IQ profile was found, but women with FXS were worse than controls only on executive function. The authors also examined which neurocognitive indices were related to the underlying biology of the disorder. Overall, the results indicated that executive rather than visuospatial deficits were primary in the neurocognitive profile of FXS.
Belser RC. Sudhalter V. Conversational characteristics of children with fragile X syndrome: repetitive speech. [Journal Article] American Journal of Mental Retardation. 106(1):28-38, 2001 January.
The production of repetitive speech during conversations was studied in people with fragile X syndrome, autistic disorder, or mental retardation not caused by fragile X. Repetitive speech was found to be more prevalent among those with fragile X compared to the control groups, especially within atypical utterances. These results suggest that the repetitive speech seen in individuals with fragile X is not the result of either general developmental delay or undiagnosed autistic disorder, and they support our hypothesis that such speech dysfluency reflects the effects of physiological arousal caused by hypersensitivity to social and sensory stimuli. Our results are interpreted within Perkins' theory of neuropsycholinguistic function
Bailey DB Jr. Hatton DD. Tassone F. Skinner M. Taylor AK. Variability in FMRP and early development in males with fragile X syndrome. American Journal of Mental Retardation. 106(1):16-27, 2001
To test the hypothesis that variability in development in fragile X syndrome is related to FMRP (the protein deficient in this syndrome expression), we studied 53 males between 23 and 98 months of age. For the entire group, which included males with either mosaism, partially methylated full mutation, and fully methylated full mutation, FMRP expression ranged from 1% to 40% and accounted for a small but significant amount of variance in level, but not rate, of total development as well as motor, social, adaptive, cognitive, and language development. For males with a fully methylated full mutation, the association was in the hypothesized direction, but not statistically significant. Findings support the hypothesized relationship between FMRP and individual capabilities but suggest that other factors also play a major role.
Duran Dominguez M. Molina Carrillo M. Fernandez Toral J. Martinez Merino T. Lopez Aristegui M. Alvarez Retuerto A. Onaindia Urquijo M. Tejada Minguez M. MOLECULAR DIAGNOSIS OF FRAGILE X SYNDROME BY POLYMERASE CHAIN REACTION: APPLICATION OF A DIAGNOSTIC PROTOCOL IN 50FAMILIES FROM NORTHERN SPAIN" , [Journal Article] Anales Espanoles de Pediatria. 54(4):331-339, 2001
BackgroundFragile X syndrome (FXS) is the most frequent hereditary cause of mental retardation. It can be diagnosed by molecular genetic techniques, but clinical suspicion is made less likely by it variable expression.ObjectiveTo assess the effectiveness of a six-item checklist in the preselection of children who are candidates for FXS genetic study.Material and methodsWe studied 70 male patients aged between 2 and 10 years with mental retardation of unknown cause. In all patients a checklist with six clinical criteria (mental retardation, history of familial mental retardation, long face, large ears, autistic-like behaviour, and attention deficit disorder with hyperactivity) measured from 0-2 points was applied and molecular genetic studies using polymerase chain reaction and Southern-blot were performed.ResultsIn 14 of the 70 children (20%) molecular study confirmed full mutation (200 CGG repeats). Ascore of six points in the test had the greatest discriminatory power and was reached by 14 patients (100%) with mutation, but only by 2of 56patients (3.5%) without mutation. The most accurate diagnostic model was the association of mental retardation, attention deficit disorder with hyperactivity, large ears and a history of familial mental retardation followed by long face and autistic-like behaviour.ConclusionThe six-item checklist improved the preselection of children with suspicion of FXS, which was later confirmed by molecular genetic techniques

Mallolas J. Duran M. Sanchez A. Jimenez D. Castellvi-Bel S. Rife M. Mila M. Implications of the FMR1 gene in menopause: study of 147 Spanish women. Menopause. 8(2):106-10, 2001
OBJECTIVE: To evaluate the relationship between the FMR1 premutation and premature ovarian failure (POF) in the Spanish population and the possible incorporation of this test in gynecological procedures for women with POF or early menopause (EM). DESIGN: Clinical and molecular genetic study. Ninety-eight premutated and six full-mutated carriers of fragile X syndrome and 43 women with POF were studied by polymerase chain reaction and Southern blot analysis for the CGG repeat expansion in the FMR1 gene. RESULTS: Among premutated carriers, 12.2% (12 of 98) presented with POF, and 15.3% (15 of 98) presented with EM. Neither POF nor EM was observed in any of the six full-mutated women. Two women of 43 from the POF population (4.65%) were carriers for the CGG premutation in the FMR1 gene. No correlation between CGG expansion size and age at menopause was found. A biased paternal origin of the premutation and a high twinning incidence was found in all premutated women, whether they had POF or not. CONCLUSIONS: Our data support the hypothesis that the FMR1 gene is one of the genes associated with POF and EM. Analysis of the CGG expansion in the FMR1 gene may be justified in women with POF and EM until the real role of the FMR1 premutation is determined.