bioquimica_1o
6
Pleasecite thi s art icle in pre ss as: Vor ugantiVS, etal.Short-term wei ghtloss in overweight/o bese low-income women imp roves pla sma zinc and metabolic syndrome risk factors. J Trace Elem Med Biol (2010), doi:10.1016/j.jtemb.2010.05.001 ARTICLE IN PRESS G Model JTE MB-2 5272; No.of P ages6 Journal of Trace Elements in Medicine and Biology xxx (2010) xxx–xxx Contents lists available at ScienceDirect Journal of Trace Elements in Medicine and Biology journal homepage: www.elsevier.de/jtemb Physiology Short-term weight loss in overweight/obese low-income women improves plasma zinc and metabolic syndrome risk factors Venkata Saroja Voruganti a,∗ , Guowen Cai b , Deborah M. Klohe c , Kristine C. Jordan d , Michelle A. Lane e , Jeanne H. Freeland-Graves c a Department of Genetics, Southwest Foundation for Biomedical Research, San Antonio, TX 78227, United States b SAS Institute, 100 SAS Campus Drive, Cary, NC 27513-2414, United States c Department of Nutritional Sciences, The University of Texas at Austin, Austin 78712, United States d Division of Nutrition, University of Utah College of Health, Salt Lake City, UT 84112, United States e Nutrition and Foods Program, Department of Family and Consumer Sciences, Texas State University, San Marcos, TX 78666, United States a r t i c l e i n f o Article history: Received 2 November 2009 Accepted 19 May 2010 Keywords: Obesity Intervention Body fat a b s t r a c t Metab olic syndr ome is a group of disorders invo lvingobesity, insulin resistance, dysl ipide mia and hype r- tension. Obesity is the most crucial risk factor of metabolic syndrome, because it is known to precede other risk factors. Obesity is also associated with disturbances in the metabolism of the trace mineral, zinc. The overall purpose of this study was to investigate the effects of short-term weight loss on plasma zinc andmetabolic syn drome ris k factors. An 8- wee k wei ghtloss int ervent ionstudywas con duc tedwith 90 low-i ncome overweigh t/obes e mothe rs, whos e young estchild was1–3 yearsold. Plas ma level s of zinc, glucose, insulin, leptin, triglycerides, total, high-density lipoprotein (HDL) and low-density lipoprotein (LDL) cholesterol were measured and compared at weeks 0 and 8 of the weight loss program. At pre- study,plas mazinc waslowin 39%and,within nor mal valuesin 46% , of obese/ overwe igh t mot her s. By the endof int ervent ion, pla sma zin c ros e by 22%and onl y 5% of themothe rs con tin uedto exh ibi t low pla sma zinc. At post-study, the metabolic syndrome risk factors of waist circumference, HDL cholesterol, and diastolic blood pressure ( p < 0.05) showed significant improvements. Plasma zinc increased by a greater margin (67%) in women with low zinc, as compared to those with normal zinc (18%); weight reduction was similar in both the groups. Finally, changes in % body fat were related negatively with changes in plasma zinc (r = − 0.28, p < 0.05). The circulating levels of zinc, as well as the meta bolic syndrome com- ponents, showed significant improvements in overweight/obese low-income women after weight loss. © 2010 Elsevier GmbH. All rights reserved. Introduction Metabolic syndrome is a group of disorders involving obesity, insulin resistance, dyslipidemia and hypertension [1]. This condi- tion affects about 35% of adults in the United States (US) [2]. An earlier study by Ford [3] f ound the prevalence of metabolic syn- drome in US adults to be approximately 27%, an increase of 16% since 1994 [3]. This escalation is particularly alarming for women, because they showed a greater increase (23.5%) than men (2.2%) [3]. Accor ding to the Nati onal Chole stero l Educa tion Progr am-Adult Treatment Panel (NCEP ATP III), metabolic syndrome is charac- terized by the presence of at least three of the following risk ∗ Corresponding author at: Department of Genetics, Southwest Foundation for Biomedical Research, PO Box 760549, San Antonio, TX 78245, United States. Tel.: +1 210 258 9795; fax: +1 210 258 9132. E-mail address: [email protected] (V.S. Voruganti). factors; waist circumference > 88cm for wome n and> 102cm for men, fast ing glucos e> 100mg/dl, fasti ng trigly cerid es > 150mg/dl, HDL cholesterol < 50 mg/dl f or women and< 40 mg/d l for men, and bloo d press ure > 130/ 85 mm Hg [4]. Although metabolic syndrome is considered to be the combined effect of all these risk factors, each individual component is known to independently augment the ris k of associate d dis eas es suc h as car dio vas cul ar dis ord ers and type 2 diabetes [5]. The recent escalation in metabolic syndrome incidence has been attributed to obesity [2], the most crucial risk factor of this syndrome [6]. The pre val enc e of obe sit y has bee n esca lat ing rap idl y; in 2007–2008 the age adjusted prevalence of obesity was 33.8% [7]. Als o, obe sit y is wid espread in women, predominantl y in those who are low-i ncome [8] and minor ity [9]. Metab olic syndr ome and obe- sity are assoc iated with several meta bolic distur bances, one of them being alterations in the metabolism of trace minerals such as zinc [10]. Zinc status, particularly circulating level, is known to be altered in conditions such as obesity and type 2 diabetes, as observed in animal [11–13] as well as human [14–16] models. 0946-672X/$ – see front matter © 2010 Elsevier GmbH. All rights reserved. doi:10.1016/j.jtemb.2010.05.001
Transcript of bioquimica_1o

8/8/2019 bioquimica_1o
http://slidepdf.com/reader/full/bioquimica1o 1/6
Please cite this article in press as: VorugantiVS, et al.Short-term weightloss in overweight/obese low-income women improves plasma
zinc and metabolic syndrome risk factors. J Trace Elem Med Biol (2010), doi:10.1016/j.jtemb.2010.05.001
ARTICLE IN PRESSG Model
JTEMB-25272; No.of Pages6
Journal of Trace Elements in Medicine and Biology xxx (2010) xxx–xxx
Contents lists available at ScienceDirect
Journal of Trace Elements in Medicine and Biology
j o u r n a l h o m e p a g e : w w w . e l s e v i e r . d e / j t e m b
Physiology
Short-term weight loss in overweight/obese low-income women improves
plasma zinc and metabolic syndrome risk factors
Venkata Saroja Voruganti a,∗, Guowen Cai b, Deborah M. Klohe c, Kristine C. Jordan d,Michelle A. Lane e, Jeanne H. Freeland-Graves c
a Department of Genetics, Southwest Foundation for Biomedical Research, San Antonio, TX 78227, United Statesb SAS Institute, 100 SAS Campus Drive, Cary, NC 27513-2414, United Statesc Department of Nutritional Sciences, The University of Texas at Austin, Austin 78712, United Statesd Division of Nutrition, University of Utah College of Health, Salt Lake City, UT 84112, United Statese Nutrition and Foods Program, Department of Family and Consumer Sciences, Texas State University, San Marcos, TX 78666, United States
a r t i c l e i n f o
Article history:
Received 2 November 2009
Accepted 19 May 2010
Keywords:
Obesity
Intervention
Body fat
a b s t r a c t
Metabolic syndrome is a group of disorders involvingobesity, insulin resistance, dyslipidemia and hyper-
tension. Obesity is the most crucial risk factor of metabolic syndrome, because it is known to precede
other risk factors. Obesity is also associated with disturbances in the metabolism of the trace mineral,
zinc. The overall purpose of this study was to investigate the effects of short-term weight loss on plasma
zinc andmetabolic syndrome risk factors. An 8-week weightloss interventionstudywas conductedwith
90 low-income overweight/obese mothers, whose youngestchild was1–3 yearsold. Plasma levels of zinc,
glucose, insulin, leptin, triglycerides, total, high-density lipoprotein (HDL) and low-density lipoprotein
(LDL) cholesterol were measured and compared at weeks 0 and 8 of the weight loss program. At pre-
study,plasma zinc was lowin 39%and,within normal valuesin 46%, of obese/overweight mothers. By the
endof intervention, plasma zinc rose by 22%and only 5% of themothers continuedto exhibit low plasma
zinc. At post-study, the metabolic syndrome risk factors of waist circumference, HDL cholesterol, and
diastolic blood pressure ( p < 0.05) showed significant improvements. Plasma zinc increased by a greater
margin (67%) in women with low zinc, as compared to those with normal zinc (18%); weight reductionwas similar in both the groups. Finally, changes in % body fat were related negatively with changes in
plasma zinc (r =− 0.28, p < 0.05). The circulating levels of zinc, as well as the metabolic syndrome com-
ponents, showed significant improvements in overweight/obese low-income women after weight loss.
© 2010 Elsevier GmbH. All rights reserved.
Introduction
Metabolic syndrome is a group of disorders involving obesity,
insulin resistance, dyslipidemia and hypertension [1]. This condi-
tion affects about 35% of adults in the United States (US) [2]. An
earlier study by Ford [3] f ound the prevalence of metabolic syn-
drome in US adults to be approximately 27%, an increase of 16%
since 1994 [3]. This escalation is particularly alarming for women,because they showed a greater increase (23.5%) than men (2.2%)
[3].
According to the National Cholesterol Education Program-Adult
Treatment Panel (NCEP ATP III), metabolic syndrome is charac-
terized by the presence of at least three of the following risk
∗ Corresponding author at: Department of Genetics, Southwest Foundation for
Biomedical Research, PO Box 760549, San Antonio, TX 78245, United States.
Tel.: +1 210 258 9795; fax: +1 210 258 9132.
E-mail address: [email protected] (V.S. Voruganti).
factors; waist circumference > 88cm for women and> 102cm for
men, fasting glucose > 100mg/dl, fasting triglycerides > 150mg/dl,
HDL cholesterol < 50 mg/dl for women and< 40 mg/dl for men, and
blood pressure > 130/85 mm Hg [4]. Although metabolic syndrome
is considered to be the combined effect of all these risk factors,
each individual component is known to independently augment
the risk of associated diseases such as cardiovascular disorders and
type 2 diabetes [5]. The recent escalation in metabolic syndromeincidence has been attributed to obesity [2], the most crucial risk
factor of this syndrome [6].
The prevalence of obesity has been escalating rapidly; in
2007–2008 the age adjusted prevalence of obesity was 33.8% [7].
Also, obesity is widespread in women, predominantly in those who
are low-income [8] and minority [9]. Metabolic syndrome and obe-
sity are associated with several metabolic disturbances, one of
them being alterations in the metabolism of trace minerals such
as zinc [10]. Zinc status, particularly circulating level, is known
to be altered in conditions such as obesity and type 2 diabetes,
as observed in animal [11–13] as well as human [14–16] models.
0946-672X/$ – see front matter © 2010 Elsevier GmbH. All rights reserved.
doi:10.1016/j.jtemb.2010.05.001

8/8/2019 bioquimica_1o
http://slidepdf.com/reader/full/bioquimica1o 2/6
Pleasecite this article in press as: Voruganti VS,et al.Short-term weightloss in overweight/obese low-income women improves plasma
zinc and metabolic syndrome risk factors. J Trace Elem Med Biol (2010), doi:10.1016/j.jtemb.2010.05.001
ARTICLE IN PRESSG Model
JTEMB-25272; No.of Pages6
2 V.S. Voruganti et al. / Journal of Trace Elements in Medicine and Biology xxx (2010) xxx–xxx
Specifically, plasma zinc has been observed to be low in obese chil-
dren and adolescents [15,16], adult men and women [17–20], and
obese mice [21].
Zinc, a trace element, is required for several cellular functions
and participates in important metabolic pathways related to the
metabolism of proteins, carbohydrates, lipids and nucleic acids
[16,22]. Zincdeficiencyhas several features in common withinsulin
resistance,hyperglycemia,and impairedglucose tolerance [10] and
maylead to the development of diabetes [23]. The influence of zinc
on glucose metabolism may be related to its insulin-like properties.
For example, zinc promotes lipogenesisand glucose transportin rat
adipocytes [24] and glucose uptake in mouse skeletal muscle [25].
Moreover, zinc may be involved in insulin signaling by forming a
complex with insulin and increasing the ability of insulin to bind
to its receptor [16]. Thus, it is conceivable that zinc may play a role
in the metabolic syndrome.
Weight lossis an effective treatmentfor the metabolic syndrome
[26] as it has been shown to improve blood pressure and plasma
concentrations of glucose, insulin and lipids [27]. Additionally,
plasma zinc also increases with weight loss. Specifically, plasma
zinclevels increasedand returned to normal levelsin obesepatients
whowere fedhypocaloricdiets [19,28]. In contrast, morbidly obese
patients undergoing a Roux-en-Y gastric bypass surgery did not
have attenuations in plasma zinc with weight loss [20]. There-fore, the effect of weight loss on circulating zinc levels remains
controversial. In the current study, the primary objective was to
investigate the effect of short-term weight loss on circulating zinc
levels. The secondary aim was to confirm the positive effects of
weight loss on metabolic syndrome risk factors.
Material and methods
Design
An 8-week weight loss intervention study was conducted with
90 overweight or obese, (body mass index (BMI) ≥25kg/m2) low-
income mothers. All participants were administered a 33-item
demographic questionnaire at week 0. Details of the interventionhave been given in Klohe-Lehman et al. [29]. In short, anthropo-
metric variables (body weight, waist circumference, percent body
fat, BMI, blood pressure) were obtained at weeks 0 and 8. Blood
was collectedaftera 12-h fasting period; plasmawas extractedand
stored at−80 ◦C untilfurtheranalysis. Plasma levelsof zinc,glucose,
insulin, leptin, triglycerides, total and high-density lipoprotein
(HDL) and low-density lipoprotein (LDL) cholesterol were mea-
sured at weeks 0 and 8.
Subjects
Selection criteria included: age, 18–45 years; youngest child,
1–3 years; Hispanic, Caucasian or African-American ethnicity;
English literacy; eligibility for WICor Medicaid; and income< 200%of the federal poverty index. The ethnicity of the participants was
63% Hispanic, 19% African-American and 18% Caucasian.The nature
of the risks and benefits of the study were explained to the partic-
ipants, and informed consent was given. The Institutional Review
Board of The University of Texas at Austin approved this study.
Anthropometric measurements
Heightwas measured in inchesusing a stadiometer (Perspective
Enterprises, Portage, MI). Weight was determined with an elec-
tronic scale (Model HS-100-A, Fairbanks Scales, St. Johnsbury, VT).
Waistcircumference was obtained by positioninga measuring tape
around the abdomen at the highest lateral border on the right
ilial crest, as recommended by NHANES III (National Heart Lung
and Blood Institute 1998). Percent body fat was estimated by bio-
electric impedance(Model TBF-300A,Tanita Corporation, Arlington
Heights, IL). Body mass index (BMI, kg/m2) wascalculated by divid-
ing body weight in kilograms by height in meters squared. Systolic
and diastolicblood pressures were measured with sphygmamome-
ter (Model Marshall Medical, Placerville, CA).
Biochemical measurements
Plasmazinc was determined by a flame atomic absorption spec-
trophotometer (5100PC, Perkin Elmer Corporation, Shelton, CT)
[30]. Plasma glucose was analyzed by a glucometer (Glucome-
ter Elite, Bayer Corporation, Elkhart, IN). Plasma concentrations
of insulin and leptin were measured using a commercial enzyme-
linked immunoabsorbent assay kit (ALPCO, Windham, NH). Lipids,
including triglycerides, total and HDL cholesterol were obtained
enzymatically (Sigma Diagnostics Inc., St. Louis, MO). The Freid-
wald formula was used to estimate LDL cholesterol [31]. Insulin
sensitivity was calculated by the Quicki method [32] and insulin
resistance was computed by the homoeostatic model assessment
method (HOMA) [33]. The prevalence of metabolic syndrome was
evaluated in these mothers, based on the criteria given in the NCEP
ATP III panel [4].
Statistical analyses
Statistical package for social sciences (SPSS, version 10.0; SPSS
Inc., Chicago, USA) was used for all statistical analyses. Descrip-
tives (means, standard deviation and range) were computed for
both anthropometric and biochemical parameters. Relationships
between zinc and other metabolic syndrome risk factors were
tested using Pearson’s correlation between anthropometric and
biochemical measurements. Analysis of variance (ANOVA) with
post hoc Scheffe analysis was used to determine significant differ-
ences between three or more subject groups. All differences were
considered to be significant at p < 0.05.
Results
At pre-study, all mothers were premenopausal and their ages
ranged from 18 to 42 years (mean 27.6±0.6 years). Based on
BMI, 22% were overweight (BMI 25–29.99 kg/m2), 56% obese (BMI
30–39.99kg/m2) and 22% were morbidly obese (BMI≥40kg/m2).
At baseline, plasma zinc was low in 39% (<0.8 mg/l) and within
normal values in 46% (0.8–1.2 mg/l) of mothers. Mothers in both
groups(lowvs. normalzinc) hadcomparableBMIsat thestart ofthe
study. For metabolic syndrome risk factors, 88%had elevated waist
circumference; 67%, high fasting glucose; 29%, enhanced triglyc-
erides; and 88%, low HDL cholesterol.
Moderate weight loss increased plasma zinc following
intervention in low-income women
At the start of this study, 39% of mothers had low plasma zinc
(<0.8mg/dl).After the 8-week intervention period, plasma zincrose
by 22% during the intervention. At the end of the study, only 5%
of the mothers continued to exhibit low plasma zinc. Weight loss
was similar in mothers with low zinc at baseline versus those who
exhibited normal zinc at baseline.
Moderate weight loss improved metabolic syndrome risk factors
following intervention in low-income women
A moderate weight loss of ∼2.3kg (2.5%) was observed in moth-
ers after an 8-week intervention program. This weight loss ranged
from 0 to 11.5 kg. Pre- and post-study characteristics (Table 1)

8/8/2019 bioquimica_1o
http://slidepdf.com/reader/full/bioquimica1o 3/6
Please cite this article in press as: VorugantiVS, et al.Short-term weightloss in overweight/obese low-income women improves plasma
zinc and metabolic syndrome risk factors. J Trace Elem Med Biol (2010), doi:10.1016/j.jtemb.2010.05.001
ARTICLE IN PRESSG Model
JTEMB-25272; No.of Pages6
V.S. Voruganti et al. / Journal of Trace Elements in Medicine and Biology xxx (2010) xxx–xxx 3
Table 1
Pre- and post-study descriptive characteristics of participating mothers.
Characteristics Pre-studya Post-studya P -value
BMIb (kg/m2) 35.4 ± 0.8a 34.6 ± 0.8a <0.001
Body fat (%) 43.2 ± 0.7 42.1 ± 0.7 <0.001
Leptin (ng/ml) 18.3 ± 1.09 18.9 ± 1.1 NS
Insulin (IU/l) 13.0 ± 1.2 14.7 ± 01.6 NS
HOMAc IR 4.0 ± 0.7 3.6 ± 0.42 NS
Cholesterol (mg/dl)
Total 166 ± 4.1 158 ± 3.3 <0.05LDLd 103 ± 4.1 87.2 ± 4.4 <0.01
Zinc (mg/l) 0.85 ± 0.04 1.04 ± 0.02 <0.001
Metabolic syndrome risk factors
Waist circumference (cm) 107 ± 2.0 104.7 ± 1.9 <0.001
Glucose (mg/dl) 112 ± 4.8 106.8 ± 4.9 NS
Triglycerides (mg/dl) 123.7 ± 7.0 115.8 ± 3.3 NS
HDLe cholesterol (mg/dl) 38.7 ± 1.2 52.3 ± 3.4 <0.0001
Blood pressure (mmHg)
Systolic 118 ± 1.4 116 ± 1.4 NS
Diastolic 77.6 ± 1.1 75.7 ± 0.9 <0.05
a Mean±SEM.b Body mass index.c Homeostatic model assessment method (Mathews et al. [33]).d Low-density lipoprotein.e High-density lipoprotein.
show significant decreases in BMI, percent body fat, BMI, total, and
LDL cholesterol, waist circumference and diastolic blood pressure
and increase in HDL cholesterol and plasma zinc. No change was
observed in plasma leptin, insulin or systolic blood pressure. The
decreases in plasma glucose and triglyceride following intervention
were not statistically significant. At the pre-intervention stage, 53%
of the participants had metabolic syndrome; whereas, only 19% of
the mothers exhibited this syndrome at post-intervention.
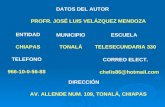
Changes in body fat were associated negatively with changes in
plasma zinc
The relationship between changesin % body fatand plasma zinc
is depicted in Fig. 1. These data show a decrease of 2.4% in body fat,
which was associated with an increase in circulating zinc (r 2 =−
0.28, p < 0.05).
Fig. 1. Relationship of changes in % body fat and changes in plasma zinc.
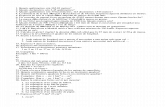
Fig. 2. Relationship of changes in dietary intakes of energy and zinc.
Changes in dietary zinc were positively associated with reduction
in energy intake
Energy and zinc intakes were evaluated pre- and post-
intervention. Mean (SE) energy intake declined from 2007 (49 kcal
at week 0 to 1465 [46] kcal, p < 0.001) at week 8. Concomitantly,
dietary zinc decreased by ∼20% during the 8-week period [mean
(SE) at week 0 = 9.22 (0.3) mg] as compared to week 8 [mean
(SE) = 7.43 (0.3)mg] p < 0.0001. The reduction in energy intake
was significantly correlated with change in dietary zinc (r 2 =0.42,
p < 0.0001) (Fig. 2).
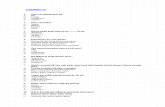
Mothers differed in their response to weight loss based on their
baseline plasma zinc status
Fig. 3 depicts the prevalence of metabolic syndrome risk factors
at pre- and post-study, in mothers with low and normal zinc lev-
elsat baseline. At baseline, mothers with lowzinc exhibitedgreater
waist circumference andpercent body fat, andhigher plasmalevels
of glucose, insulin, triglycerides and LDL cholesterol as compared
to those with normalzinc; howeverthese differences were not sta-
tistically significant ( p > 0.05). Although weight loss was similar in
both groups, mothers with lowzincat baseline showeda significant
decrease in waist circumference and plasma glucose than mothers
who had normal zinc at baseline. Plasma zinc levels increased in
both groups; interestingly the increase was more pronounced in
mothers with low baseline zinc than others. Percent body fat, body
mass index and HDL cholesterol showed similar improvements inboth groups (Fig. 3).
Discussion
A modest reduction in weight and metabolic risk factors is
knownto dramatically enhance well-beingand improve health sta-
tus [34]. In addition, moderate weight loss can improve glycemic
control and insulin sensitivity in type 2 diabetic patients and pre-
vent the progression to diabetes in patients who are at high risk.
In the current study, small weight loss normalized plasma zinc and
diminished risk factors for metabolic syndrome. Specifically, lower
zinc levels at pre-intervention were associated with greater post-
intervention decreases in plasma glucose and blood pressure, as
well as increased HDL and plasma zinc. This response is encourag-

8/8/2019 bioquimica_1o
http://slidepdf.com/reader/full/bioquimica1o 4/6
Pleasecite this article in press as: Voruganti VS,et al.Short-term weightloss in overweight/obese low-income women improves plasma
zinc and metabolic syndrome risk factors. J Trace Elem Med Biol (2010), doi:10.1016/j.jtemb.2010.05.001
ARTICLE IN PRESSG Model
JTEMB-25272; No.of Pages6
4 V.S. Voruganti et al. / Journal of Trace Elements in Medicine and Biology xxx (2010) xxx–xxx
Fig. 3. Metabolic risk factors at pre-and post-study in mothers withbaselinelow and normal plasma zinc.Black and whitebars indicate pre-and post-study measurements,
respectively.
ing, as many individuals findit difficult to lose substantial amounts
of weight.
Metabolic syndrome is a complex, multifactorial disorder, with
obesity being the primary risk factor. Thus weight loss is the first
and foremost therapy that should be adopted for treating this
condition, followed by treatment of individual components of the
syndrome [35]. In the present study a modest weight loss of 2.5%
occurred. However, this minimal weightloss reduced the incidence

8/8/2019 bioquimica_1o
http://slidepdf.com/reader/full/bioquimica1o 5/6
Please cite this article in press as: VorugantiVS, et al.Short-term weightloss in overweight/obese low-income women improves plasma
zinc and metabolic syndrome risk factors. J Trace Elem Med Biol (2010), doi:10.1016/j.jtemb.2010.05.001
ARTICLE IN PRESSG Model
JTEMB-25272; No.of Pages6
V.S. Voruganti et al. / Journal of Trace Elements in Medicine and Biology xxx (2010) xxx–xxx 5
of metabolic syndrome by one-third. Beneficial changes also were
observed in individual risk factors such as waist circumference, cir-
culating glucose, triglycerides and HDL cholesterol. For comparison
the prevalence of metabolic syndrome was decreased by 59% after
a weight loss of 8.2 kg (∼8%) in older obese adults [36]. However,
more modest weight losses also have been reported to improve
metabolic risk factors. A study conducted by Lofgren et al. [37]
found that a 5% weight loss reversed metabolic syndrome in seven
out of eight premenopausal women.
Low plasma zinc levels have been observed in obese [19,28],
type 2 diabetic [22] and obese-type 2 diabetic individuals [14,38].
Similarly, low plasma zinc (<0.8 mg/dl) was observed in 39% of the
overweight/obese women in the current study. Ninety percent of
these values returned to normal with weight loss. Woodhouse et
al. [19] also found a rise in plasma zinc (7%), with a 5.9% decrease
in weight of men and women fed a high dairy hypocaloric diet for
12 weeks. Similarly, Di Martino et al. [17] reported elevated plasma
zinc of 16% in men and 33% in women whose BMI had declined by
an average of 15%decline. In a Japanese weight loss program based
on hypocaloric diets, weight loss was associated with increased
plasma zinc [28]. The same response has been observed in obese
children and adolescents; plasma zinc escalated by 12% after 10
weeks of consuming a very low calorie diet [15]. In contrast, one
1987 study by Brighenti et al. did not show any improvement inplasma zinc status with weight loss in obese subjects [39]. In the
present study, plasma zinc was elevated by about 9% for every 1%
of the body weightlost.Whether or notplasma zinc levels returnto
low baseline concentrations with time merits further investigation.
In this paper, an increase in plasma zinc was associated with a
decrease in % body fat. This increase was not reflective of diet, as
dietary levels of zinc declined by 20%; this decline presumably was
due to the reduction in calories that occurred as a consequence of
dieting. In another study, women judo athletes undergoing physi-
cal training, plasma zinc was inversely associated with % body fat
as also observed in our research [40]. In a cross-sectional study
in Indian men, higher body fat percent was associated with lower
concentrations of plasma zinc [41]. In normal weight humans, zinc
deficiency also was observed in conjunction with low concentra-tions of leptin, a hormone produced in adipose tissue. In obese men
(n =5), Chen et al. [42] reported an inverse relationship between
levels of zinc and leptin. In contrast, a positive relationship was
reported between plasma zinc and leptin in male athletes [43].
However, no association was observed between plasma levelof lep-
tin and zinc in the current study. These conflicting results may be
due to differences in sample size, age, sex and type of adiposityand
physical activity.
Disturbances in zincconcentrations(both circulating and tissue)
have been reported in obesity and insulin resistance. In a random-
ized placebo-controlled, cross-over studyin 60 obese children, zinc
supplementation significantly attenuated plasma levels of glucose
and insulin and HOMA [44]. Assiri et al. observed that women with
metabolic syndrome had lower levels of plasma zinc, as comparedto women without metabolic syndrome [45]. On the other hand,
men and women with metabolic syndrome were found to be at a
higher risk for zinc deficiency, although no statistical correlation
was found between plasma zinc and metabolic syndrome compo-
nents [46].
In the current study women with low plasma zinc had higher
body weight, waist circumference, plasma glucose and % body
fat than those with normal levels of this trace mineral. This is
notable since all these traits are directly or indirectly related to
metabolic syndrome. Improvements in these metabolic risk fac-
tors were more pronounced in women with low zinc than those
with normal zinc, despite similar reductions in weight. In addition,
womenwith lower plasma zinc concentration at baseline exhibited
greater increases in plasmazinc. This outcome suggests that differ-
ent homeostatic adjustments in zinc metabolism maybe dependent
on initial zinc status or related factors, rather than just weight loss
alone.
A limitation is the short duration of the present research. In a
more extended period of time, it would have been advantageous
to confirm the research findings but this was precluded by cost
and subject availability. Although studies reported here have used
plasma zinc to assess body zinc status, its reliability as an indicator
of zinc status is subject to debate. Nonetheless, a systematic review
of methods of zinc assessment in humans concluded that plasma
zinc, if collected and stored properly, could be a reliable indicator
of body zinc status [47]. Thus the changes observed in plasma zinc
might be a reflection of changes in body zinc status [48].
In summary, at pre-study 53% of the overweight or obese low-
income women exhibited risk factors for metabolic syndrome, and
39%had lowconcentrations of plasmazinc.The circulating levelsof
zinc, as well as the metabolic syndrome components, showed sig-
nificant improvements in overweightor obeselow-income women.
These results suggest that even a moderate weight loss can confer
health benefits, irrespective of the initial weight status.
Acknowledgement
This research is supported by a grant from the Texas Higher
Education Coordinating Board, Austin, TX (UTA #00-377).
References
[1] Hansen BC. The metabolic syndrome X. N Y Acad Sci 1999;892:1–24.[2] Ford ES. Prevalence of the metabolic syndrome defined by the International
Diabetes Federation among adults in the U.S. Diabetes Care 2005;28:2745–9.[3] Ford ES. Prevalence of the metabolic syndrome in US populations. Endocrinol
Metab Clin Am 2004;33:333–50.[4] Grundy SM, Brewer Jr HB, Cleeman JI, Smith Jr SC, Lenfant C. Definition of
metabolic syndrome: report of the National Heart, Lung, and Blood Insti-tute/American Heart Association conference on scientific issues related todefinition. Circulation 2004;109:433–8.
[5] Bosello O, Zamboni M. Visceral obesity and metabolic syndrome. Obesity Rev2000;1:47–56.
[6] Lemieux S. Contribution of visceral obesity to the insulin resistance syndrome.Can J Appl Physiol 2001;26(3):273–90.
[7] Flegal KM, Carroll MD, Ogden CL, Curtin LR. Prevalence and trends in obesityamong US adults, 1999–2008. JAMA 2010;303:235–41.
[8] Breitkopf CR, Berenson AB. Correlates of weight loss behaviors among low-income African-American, Caucasian and Latina women. Obstet Gynecol2004;103:231–9.
[9] CossrowN, Falkner B. Race/ethnic issues in obesity and obesity-related comor-bidities. J Clin Endocrinol Metab 2004;89:2590–4.
[10] Tallman DL, Taylor CG. Effects of dietary fat and zinc on adiposity, serumleptin, and adipose fatty acid composition in C57BL/6J mice. J Nutr Biochem2003;14:17–23.
[11] Chen MD, Lin P-Y, Cheng V, Lin WH. Zinc supplementation aggravates bodyfat accumulation in genetically obese mice and dietary-obese mice. Biol TraceElem Res 1996;52:125–32.
[12] Blonstein-Fujji A, DiSilvestro RA, Frid D, Katz C, Malarkey W. Short-term zincplasma 5-nucleosidase activities, insulin-like growth factor1 concentrationsand lipoprotein oxidation rates in vitro. Am J Clin Nutr 1997;66:639–42.
[13] Simon SF, Taylor CG. Dietary zinc supplementation attenuates hyperglycemia
in db/db mice. EBM 2001;226:43–51.[14] KonukogluD, TurhanMS, Ercan M, Serin O. Relationshipbetweenplasma leptin
and zinc levels and the effect of insulin and oxidative stress on leptin levels inobese diabetic patients. J Nutr Biochem 2004;15:757–60.
[15] Di Toro A, Marotta A, Todisco N, Ponticiello E, Collini R, Di Lascio R, et al.Unchanged iron and copper and increased zinc in the blood of obese childrenafter two hypocaloric diets. Biol Trace Elem Res 1997;57:97–104.
[16] MarrieroDN, FisbergM, CozzolinoSMF. Zincnutritional status andits relation-ships withhyperinsulinemia in obese children andadolescents. BiolTraceElemRes 2004;100:137–49.
[17] Di Martino G, Matera MG, De Martino B, Vacca C, Di Martino S, Rossi F. Rela-tionship between zinc and obesity. J Med 1993;24:177–83.
[18] Ozata M, Mergen M, Oktenli C, Avdin A, Sanisoglu SY, Bolu E, et al.Increased oxidative stress and hypozincemia in male obesity. Clin Biochem2002;35:627–31.
[19] Woodhouse LR, Gertz ER, Radak TL, Teegarden D, Zemel MB, Van Loan MD.Effect of short-term weight losson zinc status in overweight adults consuminghypocaloric diets with high dairy intake, low dairy intake or calcium supple-
mentation. J Trace Elem Exp Med 2004;17:211.

8/8/2019 bioquimica_1o
http://slidepdf.com/reader/full/bioquimica1o 6/6
Pleasecite this article in press as: Voruganti VS,et al.Short-term weightloss in overweight/obese low-income women improves plasma
zinc and metabolic syndrome risk factors. J Trace Elem Med Biol (2010), doi:10.1016/j.jtemb.2010.05.001
ARTICLE IN PRESSG Model
JTEMB-25272; No.of Pages6
6 V.S. Voruganti et al. / Journal of Trace Elements in Medicine and Biology xxx (2010) xxx–xxx
[20] Cominetti C, Garrido Jr AB, Cozzolino SM.Zinc nutritional status of morbidlyobese patientsbeforeand after Roux-en-Y gastric bypass:a preliminary report,vol. 16. 2006. p. 448–53.
[21] ChenMD, Lin P-Y.Zinc-induced hyperleptinemia relates to the amelioration of sucrose-induced obesity with zinc repletion. Obes Res 2000;8:525–9.
[22] Song Y, Wang J, Li XK, Cai L. Zinc and the diabetic heart. Biometals2005;18:325–32.
[23] Kechrid Z, Bouzerna N. Effect of zinc deficiency and experimental diabetes onglutamate oxaloacetate, glutamate pyruvate aminotransferases and alkalinephosphatase activities in rats. Int J Diabetes Metab 2004;11:14–8.
[24] Ilouz R, Kaidanovich O, Gurwitz D, Eldar-Finkelman H. Inhibition of glyco-
gen synthase kinase-3 by bivalent zinc ions: insight into the insulin-mimeticaction of zinc. Biochem Biophys Res Commun 2002;295:102–6.
[25] MirandaER, DeyCS. Effect of chromiumand zincon insulin signaling in skeletalmuscle cells. Biol Trace Elem Res 2004;101:19–36.
[26] Bray GA. Medical consequences of obesity. J Clin Endocrinol Metab2004;89:2583–9.
[27] Aronne LJ, Segal KR. Adiposity and fat distribution outcome measures: assess-ment and clinical implications. Obes Res 2002;10:14S–20S.
[28] Ishikawa Y, Kudo H, Kagawa Y, Sakamoto S. Increased plasma levels of zinc inobese adult females on a weight-loss programbased on a hypocaloric balanceddiet. In Vivo 2005;19:1035–7.
[29] Klohe-Lehman DM, Freeland-Graves J, Clarke KK, Cai G, Voruganti VS, MilaniTJ, et al. Low-income, overweight and obese mothers as agents of change toimprove food choices, fat habits, and physical activity in their 1-to-3-year-oldchildren. J Am Coll Nutr 2007;26:196–208.
[30] Hackley BM, Smith JC,HalstedJA. A simplifiedmethod of plasmazinc determi-nation by atomic absorption spectrophotometry. Clin Chem 1967;14:1–5.
[31] Cantin B, LamarcheB, DespresJP, Dagenais GR.Does correctionof thefriedwaldformula using lipoprotein (a) change our estimation of ischemic heart disease
risk? The Quebec Cardiovascular Study. Atherosclerosis 2002;163:261–7.[32] Katz A, Nambi SS, Mather K, Baron AD, Follmann DA, Sullivan G, et al. Quanti-
tative insulin sensitivity check index: a simple, accurate method for assessinginsulin sensitivity in humans. J Clin Endocrinol Metab 2000;85:2402–10.
[33] MathewsDR,HoskerJP,Rudensky AS,NaylorBA,TreacherDF, TurnerRC. Home-ostasismodel assessment:insulinresistanceand betacell functionfrom fastingglucose and insulin concentrations in man. Diabetologia 1985;28:412–9.
[34] KleinS, SheardNF,Pi-Sunyer X, DalyA, Wylie-RosettJ, Kulkarni K,et al.Weightmanagement through lifestyle modification for the prevention and manage-ment of type 2 diabetes: rationale and strategies. A statement of the AmericanDiabetesAssociation, the North American Association for the Study of Obesity,andthe AmericanSocietyfor ClinicalNutrition.Am J ClinNutr2004;80:257–63.
[35] DeedwaniaPC, Gupta R.Managementissuesin themetabolic syndrome. J AssocPhysicians India 2006;54:797–810.
[36] Villareal DT, Miller 3rd BV, Banks M, Fontana L, Sinacore DR, et al. Effect of lifestyle intervention on metaboliccoronaryheart disease risk factors in obeseolder adults. Am J Clin Nutr 2006;84:1257–8.
[37] LofgrenIE, HerronKL, West KL,ZernTL, Brownhill RA, IlichJZ, etal. Weightlossfavorably modifies anthropometrics and reverses the metabolic syndrome inpremenopausal women. J Am Coll Nutr 2005;24:486–93.
[38] Kazi TG, Afridi HI, Kazi N, Jamali MK, Arain MB, Jalbani N, et al. Copper,chromium, manganese, iron, nickel and zinc levels in biological samples of diabetes mellitus patients. Biol Trace Elem Res 2008;122:1–18.
[39] BrighentiF, Testolin G, GiaccaA, CaviazelF, Pozza G.Dietary seleniumand zincintake and the medium-term Se and Zn status in obese persons on low-caloriediets. Int J Vitam Nutr Res 1987;57:185–92.
[40] Koury JC, de Oliviera K deJ, Lopes GC, de Oliviera Jr AV, Portella ES, de MouraEG, et al. Plasma zinc, copper, leptin and body composition are associated inelite female judo athletes. Biol Trace Elem Res 2007;115:23–30.
[41] Singh RB, Beegom R, Rastogi SS, Gaoli Z, Shoumin Z. Association of low plasmaconcentrations of antioxidant vitamins, magnesium and zinc with high bodyfatpercentmeasured by bioelectric impedanceanalysis in Indian men.MagnesRes 1998;11:3–10.
[42] Chen MD, Song YM, Lin PY. Zinc may be a mediator of leptin production inhumans. Life Sci 2000;66:2143–9.
[43] Casimiro-Lopes G, de Olibeira-Junior AV, Prtella ES, Lisboa PC, Donangelo CM,de Moura EG, et al. Plasma leptin, plasma zinc and plasma copper are asso-ciated in elite female and male judo athletes. Biol Trace Elem Res 2009;127:109–15.
[44] Hashemiopour M, Kelishadi R, Shapouri J, Sarrafzadegan N, Amini M, TavakoliN, et al. Effect of zinc supplementation on insulin resistance and componentsof the metabolic syndromein prepubertal obese childrem.Hormones(Athens)
2009;8:279–85.[45] Assiri AM, Ramadan KS, Mahfouz MH. Some biochemical changes in post-
menopausal women with and without metabolic syndrome. Egypt J BiochemMol Biol 2008;26:67–84.
[46] ObeidO, ElfakhaniM, HlaisS, IskandarM, BatalM, MouneimmeY, etal. Plasmacopper, zinc, and selenium levels and correlates with metabolic syndromecomponents of Lebanese adults. Biol Trace Elem Res 2008;123:58–65.
[47] Lowe NM, Fekete K, Decsi T. Methods of assessment of zinc status in humans:a systematic review. Am J Clin Nutr 2009;89(Suppl.):2040S–51S.
[48] Lowe NM, WoodhouseLR, Sutherland B, Shames DM, BurriBJ, Abrams SA,et al.Kinetic parameters and plasma zinc concentration correlate well with net lossand gain of zinc from men. J Nutr 2004;134:2178–81.