Polypill – ¿una solución para la falta de adherencia ... · adherencia en la prevención...
37
Polypill – ¿una solución para la falta de adherencia en la prevención cardiovascular? José R. González Juanatey Servicio de Cardiología y UCC Hospital Clínico Universitario. IDIS Santiago de Compostela Societat Catalana de Farmacia Clínica. 2017
Transcript of Polypill – ¿una solución para la falta de adherencia ... · adherencia en la prevención...

Polypill – ¿una solución para la falta de adherencia en la prevención
cardiovascular?
José R. González JuanateyServicio de Cardiología y UCC
Hospital Clínico Universitario. IDISSantiago de Compostela
Societat Catalana de Farmacia Clínica. 2017

Disclosures:Research Grants: AZ, Boehringer Ingelheim, Pfizer, Novartis, Daichii-Sankyo, Sanofi-Aventis, Bayer, MSD, Servier, FerrerConsultant/Honorarium. AZ, Boehringer-Ingelheim, Bayer, Pfizer, BMS, MSD, Daichii-Sankyo, Servier, Menarini, Ferrer, Angem

IHD 2ªPrev. An Extraordinary Journey
Innovation Year Impact
B-Blockers 70´ Mortality
ASA 80´ Mortality
Life-style changes/Rehab 70-15´ Mortality
ACE Ih 80-90´ Morbi-mortality
Statins 90´ Morbi-Mortality
Empaglifocin/Liragutide 16´ Morbi/mortality
Revasc (subgroups) 00´ Morbi-mortality
Vorapaxar 13´ Morbi-mortality
Rivaroxaban 13´ Morbi-mortality
Ticagrelor 15´ Morbi-mortality
Ezetimibe 15´ Morbi-mortality
10%/y
2%/y

Potential Cumulative Impact of 4 Simple Secondary Prevention Treatments
Risk Factors Control and Direct CV and Kidney Protection
RRR Event rate
None 8%
ASA 25% 6%
β-Blockers 25% 4.5%
Lipid lowering 30% 3.0%
ACE-inhibitors 25% 2.3%
CUMULATIVE BENEFITS ARE LIKELY TO BE IN EXCESS OF75% RRR, WHICH IS SUBSTANTIAL

Rationale for the selection of “Polypill” components forsecondary prevention
.;
ATORVASTATIN 20mg• 43% RRR of total mortality• 52% RRR of non fatal MI• 47% RRR of coronary mortality• 47% RRR of strokeAtorvastatin SmPC. GREACE study. Athyros GV.. Curr Med Res Opinion 2002. 220-228
ACETYLSALCYLIC ACID 100mg • 22% RRR of stroke• 20% RRR of coronary eventsAT trialists collaboration. Baignent. BMJ 2002;324:71-86
RRR: relative risk reduction
RAMIPRIL 10mg• 26% RRR of cardiovascular death• 20% RRR of AMI • 31% RRR of strokeHOPE Yusuf S et al. NEJM 2000;342(3):145-53

OR
* p=0.005
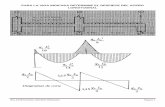
Composite outcome
%
0,11
0,7
0,5
0,9
Cardiovascular death
%
0,11
0,7
0,5
0,9
Myocardial infarction
%
0,11
0,7
0,5
0,9
New heart failure onset
%
0,11
0,7
0,5
0,9
All-cause death
%
0,11
0,7
0,5
0,9
OR
Stroke
%
0,11
0,7
0,5
0,9*
** *
*
New diabetes onset
%
0,11
0,7
0,5
0,9
** * *
ACE-Is
ARBs
* outcome significantly reduced as compared to placebo (p<0.005)
Main results
Savarese G, et al. JACC 2013; 61: 131-142

J.R.G. JUANATEY C.H.U.Santiago
Picking PlaquesThat Pop!
Narula & DeMariaJ Am Coll Cardiol
[Editorial] 2005
From Virmani, Narula, Leon, Willerson; The Vulnerable Atherosclerotic Plaques: 2007

J.R.G. JUANATEY C.H.U.Santiago
LDLc reduction and CV Protection
Ballantyne CM. Am J Cardiol 1998; O’Keefe JH et al, JACC 2004
LDL cholesterol achieved
Pati
ents
wit
h CH
D ev
ent
(%)
25
20
15
10
5
050 70 90 110 130 150 170 190 210
WOSCOPS-P
WOSCOPS-S
AFCAPS-PAFCAPS-S
LIPID-SCARE-S
4S-S
CARE-P
LIPID-P
4S-P
30
mg/dL
HPS-P
HPS-S LIPS-P
ASCOT-S
ASCOT-PLIPS-S
2° prevention statin
2° prevention placebo
1° prevention statin
1° prevention placebo
PROVE-IT APROVE-IT P
TNT 80
TNT 10AtoZ 20
AtoZ 80

Kotseva et al. J Am Coll Cardiol. 2015;66:1634-1636.
Evidence based treatments in EUROASPIRE

WHY ARE WE FAILING TO IMPLEMENT KNOWLEDGE:
A GLOBAL GAP IN TREATMENT OF CARDIVOVASCULAR DISEASE
Knowledge Implementation
System
Accessibility
Physician
Adherence
Patient
Adherence

Medication Non-Adherence
“Adherence is the degree to which a person’s behavior in
taking medication corresponds with agreed recommendations from a health care provider”
ADHERENCE TO LONG TERM THERAPIES: EVIDENCE FOR ACTION. WHO 2003

10,1
21,4
34,6
59,2
74,4
4,28,9
20
40,2
65,2
0
10
20
30
40
50
60
70
80
45-54 55-64 65-74 75-84 85-94
Men Women
Importance of Age on Adherence to Cardiovascular Medications
Incidence (%) of Cardiovascular Disease by sex and age
40% over 65 take over 4 pills
Go A. et al. AHA Statistical Update, Circulation, 2013; 129, 24-292Haider SI et al. International Journal of Clinical Pharmacology and Therapeutics, 2007 45 (12): 643–653.

Direct association between dosing frequency and medication adherence
Claxon et al, Clinical Therapeutics, 2001. Vol 23, 8: 1296-1310
79
6965
51
74
58
46
40
30
40
50
60
70
80
90
1 2 3 4
Took doses (%) Took on time (%)
% A
dher
ence SECONDARY
PREVENTION

Cholesterol
Diabetes (type 2)
Obesity
Hypertension
Treatment area 3 months 6 months 12 months
60%
52%53%
41%38%
48%
8%
47%
35%
Adherence drops after first six months
34%
By the end of the first yearof treatment, 50-90% of patients stopped taking
their prescribedmedications
Castellano JM, et al. , Global Heart. 2013 ;8:263
43%
41%

Chowdhury R et al. EHJ, 2013;34(38):2940-8.
n=1,978,919 (135,627 CVD events and 94,126 cases of all-cause mortality)
Prevalence of Good Adherence to CV Medications
Adherence to any CVD Medication
Adherence to STATINS
Adherence to ANTIHYPERTENSIVES
Adherence to ASPIRIN
Adherence to ANTIDIABETIC AGENTS
34
12
11
2
2
1.230.382
771.323
363.819
11.068
1112
0,60 (0,52-0,68)
0,54 (0,41-0,67)
0,54 (0,42-0,77)
0,70 (0,49-0,91)
0,69 (0,59-0,78)
0 0.2 0.4 0.6 0.8 1Prevalence of Good Adherence (%)
No. ofStudies
No. ofParticipants Proportion (95% CI)

Time to Major cardiac Event by Adherence Levels
Bansilal S, Castellano JM, Fuster V et al, . J Am Coll Cardiol. 2016 Aug 23;68(8):789-801
24%
44%

Adherence Levels and MACE(Hospitalizations per 100 Patient – years)
Bansilal S, Castellano JM, Fuster V et al, . J Am Coll Cardiol. 2016 Aug 23;68(8):789-801

Impact on Health Care Costs
Iuga A. et al. Risk Management and Health Care Policy. 2014:7 35-44
Medication Non-Adherence
Poor Medication Adherence
Poor Health Outcomes
Increased Service
Utilization
Increased Health Care
Costs
Costs passed on to patient

Impact on Health Care Costsn=137227 DM, HT, Hchol, CHF
Sokol M et al 2005 Medical Care. 43(6):521-530..
15186
11200 11008
9363
6377
0
2000
4000
6000
8000
10000
12000
14000
16000
0-19 20-39 40-59 60-79 80-100
Medication Non-Adherence
Adherence levels (%PDC)
Dire
ct C
osts
(USD
)

Adherence to Medication in the GuidelinesFrom “get on with the guidelines” to “strategies to improve adherence”

Polypill for Cardiovascular PreventionFrom Research to Clinical Practice
IncreasesPatient/Phys
icianCompliance
Improvesaccesibility to
provenmedication
Reduces Health Care
Costs

RCTS USING A POLYPILL TO STUDY THE EFFECT ON ADHERENCE
47
70
0102030405060708090
100
Control Polypill
46
81
0102030405060708090
Control Polypill
60
85
0102030405060708090
Control PolypillSelak et al. BMJ . 2014
Patel et al. European Journal of Preventive Cardiology, 2014
Thom S, et al. JAMA . 2013;310:918-929
KANYINI GAP IMPACT UMPIRERR=1,49 RR=1,75 RR=1,33
Castellano JM et al, J Am Coll Cardiol. 2014;64(6):613-621


Attending Visit 3+ MAQ=20+Pill Count 80-110 Attending all visits+MAQ=20+Pill Count 80-110
p=0.019p=0.012
10% adherence increase with the CNIC-Ferrer polypill (Trinomia ASR) in patients with long-term evaluated CV disease
FOCUS Project: Phase 2, Results
Castellano JM et al. A Polypill Strategy to Improve Adherence: Results From the FOCUS Project. J Am Coll Cardiol. 2014 Sep 1.pii: S0735-1097(14)05941-5. doi: 10.1016/j.jacc.2014.08.021 .


Poor adherence leads to poor outcomes and a polypill strategy leads to better adherence. Hence
the implementation of a polypill strategy in post MI setting should lead to better clinical outcomes.
Hypothesis
Confidential | For internal and investigator use only

n=3200Post MI >65
MACECardiovascular deathNonfatal myocardial infarctionNonfatal ischemic strokeUrgent revascularization
FU: 2-4 years
Study Overview
Confidential | For internal and investigator use only

Confidential | For internal and investigator use only
n=600
n=600
n=400
n=700
n=250
n=250
n=400
Partners | Inclusion

A step ahead in secondary prevention of cardiovascular risk
Consensus document on clinical use of the polypill



The “New Polypill” for Cardiovascular PreventionFrom Hospital to Outpatient Care
IncreasesPatient/Physician Compliancefrom Hospital
Discharge
Improvesaccesibilityto proven
medication
Reduces Health Care
Costs
Atorvastatin40 mgs


Halvorsen S et al JACC 2014; 64:319 - 327



WHY ARE WE FAILING TO IMPLEMENT KNOWLEDGE: A GLOBAL GAP IN TREATMENT OF CARDIVOVASCULAR DISEASE
Knowledge Implementation
“Increasing the effectiveness of adherence interventions may have a far greater impact on the health of the population than
any improvement in specific medical treatments”



![[THE GREATER MANCHESTER]...Espai de coneixement i debat sobre temes metropolitans – The Greater Manchester 3 1 Presentació Després d’una primera trobada dedicada al Gran París,](https://static.fdocuments.mx/doc/165x107/5e51d6cb727a6152bf3ae3d6/the-greater-manchester-espai-de-coneixement-i-debat-sobre-temes-metropolitans.jpg)