La retinopatía severa del prematuro predice maduración ...a_severa_del... · Steven P Miller...
18
La retinopatía severa del prematuro predice maduración demorada de sustancia blanca y pobre neurodesarrollo Torin J A Glass, Vann Chau, Jane Gardiner, Justin Foong, Jillian Vinall, Jill G Zwicker, Ruth E Grunau, Anne Synnes, Kenneth J Poskitt, Steven P Miller RESUMEN Objetivo Determinar si la retinopatía del prematuro (ROP) severa está asociada con (1) anormal maduración de la sustancia blanca y (2) los resultados de neurodesarrollo (ND) a los 18 meses de edad corregida (EC) comparados con neonatos sin ROP severa. Diseño Cohorte longitudinal prospectiva de neonatos extremadamente prematuros (EPT) nacidos a las 24-28 semanas de edad gestacional (EG) reclutados entre 2006 y 2013 con RNMs de cerebro obtenidas temprano en la vida y en la edad equivalente al término. ROP severa fue definida como ROP tratada con fotocoagulación láser de retina. Utilizando imágenes de tensor de difusión y estadísticas espaciales basadas en el tracto (TBSS), se evaluó la maduración de la sustancia blanca por medio de anisotropía fraccional (AF) en siete regiones predefinidas de interés. Los resultados de ND se evaluaron con scores compuestos de la escala Bayley-III a los 18 meses de EC. Los sujetos se compararon usando Test exacto de Fisher, Kruskal Wallis y ecuaciones de estimación generalizadas. Ámbito Las familias se reclutaron de la UCIN del BC Women´s Hospital. Pacientes De 98 RN EPT (mediana: 26.0 semanas) evaluados localmente para ROP, 19 (19%) tuvieron ROP severa y 83 (85%) fueron evaluados a los 18 meses de EC. Resultados La ROP severa estuvo asociada con AF más baja en la sustancia blanca posterior, y con medidas de maduración cerebral disminuidas en las radiaciones ópticas, brazo posterior de la cápsula interna (PLIC) y cápsula externa en TBSS. Los scores cognitivos y motores fueron más bajos en infantes con ROP severa. Conclusiones La ROP severa está asociada con retraso de la maduración de las radiaciones ópticas, PLIC, cápsula externa y posterior de sustancia blanca, que albergan los pasos visual primario y motor, y está asociada con resultados cognitivos y motores a los 18 meses de EC. ¿Qué se sabe sobre este tema? ➢ La retinopatía severa de la prematurez (ROP) es una alteración retiniana potencialmente desvastante del infante prematuro que puede ser tratada con fotocoagulación retiniana para preservar la visión ➢ ROP severa está asociada con pobres resultados del ND pese a resultados visuales favorables. ¿Qué agrega este estudio? ➢ Los scores cognitivos y motores a los 18 meses de EC estuvieron preferentemente impactados en niños con ROP severa ➢ La maduración de sustancia blanca en el extremo posterior de la cápsula interna, cápsula externa y radiaciones ópticas estuvo demorado en infantes con ROP severa
Transcript of La retinopatía severa del prematuro predice maduración ...a_severa_del... · Steven P Miller...

La retinopatía severa del prematuro predice maduración demorada de sustancia
blanca y pobre neurodesarrollo
Torin J A Glass, Vann Chau, Jane Gardiner, Justin Foong, Jillian Vinall, Jill G Zwicker, Ruth E Grunau,
Anne Synnes, Kenneth J Poskitt,
Steven P Miller
RESUMEN
Objetivo Determinar si la retinopatía del prematuro (ROP) severa está asociada con (1) anormal
maduración de la sustancia blanca y (2) los resultados de neurodesarrollo (ND) a los 18 meses de
edad corregida (EC) comparados con neonatos sin ROP severa.
Diseño Cohorte longitudinal prospectiva de neonatos extremadamente prematuros (EPT) nacidos
a las 24-28 semanas de edad gestacional (EG) reclutados entre 2006 y 2013 con RNMs de cerebro
obtenidas temprano en la vida y en la edad equivalente al término. ROP severa fue definida como
ROP tratada con fotocoagulación láser de retina. Utilizando imágenes de tensor de difusión y
estadísticas espaciales basadas en el tracto (TBSS), se evaluó la maduración de la sustancia blanca
por medio de anisotropía fraccional (AF) en siete regiones predefinidas de interés. Los resultados
de ND se evaluaron con scores compuestos de la escala Bayley-III a los 18 meses de EC. Los sujetos
se compararon usando Test exacto de Fisher, Kruskal Wallis y ecuaciones de estimación
generalizadas.
Ámbito Las familias se reclutaron de la UCIN del BC Women´s Hospital.
Pacientes De 98 RN EPT (mediana: 26.0 semanas) evaluados localmente para ROP, 19 (19%)
tuvieron ROP severa y 83 (85%) fueron evaluados a los 18 meses de EC.
Resultados La ROP severa estuvo asociada con AF más baja en la sustancia blanca posterior, y
con medidas de maduración cerebral disminuidas en las radiaciones ópticas, brazo posterior de
la cápsula interna (PLIC) y cápsula externa en TBSS. Los scores cognitivos y motores fueron más
bajos en infantes con ROP severa.
Conclusiones La ROP severa está asociada con retraso de la maduración de las radiaciones
ópticas, PLIC, cápsula externa y posterior de sustancia blanca, que albergan los pasos visual
primario y motor, y está asociada con resultados cognitivos y motores a los 18 meses de EC.
INTRODUCCIÓN
¿Qué se sabe sobre este tema?
➢ La retinopatía severa de la prematurez
(ROP) es una alteración retiniana
potencialmente desvastante del infante
prematuro que puede ser tratada con
fotocoagulación retiniana para preservar la
visión
➢ ROP severa está asociada con pobres
resultados del ND pese a resultados
visuales favorables.
¿Qué agrega este estudio?
➢ Los scores cognitivos y motores a los 18
meses de EC estuvieron
preferentemente impactados en niños
con ROP severa
➢ La maduración de sustancia blanca en
el extremo posterior de la cápsula
interna, cápsula externa y radiaciones
ópticas estuvo demorado en infantes
con ROP severa

La ROP es un desorden proliferativo de la vascularización retiniana que es más severo en
neonatos EPT nacidos <28 semanas de EG. Las estrategias terapéuticas primarias para ROP
incluyen prevención del desarrollo anormal de los vasos con estricto control de la oxigenoterapia
suplementaria y, cuando es severo, tratamiento con fotocoagulación láser de retina o más
recientemente factor de crecimiento endotelial antivascular intravítreo (anti- VEGF) (1, 2).Varios
estudios de extensas cohortes de neonatos PT han mostrado que la ROP severa está asociada con
scores cognitivos y motores más bajos en la infancia temprana (3-6). Pese a resultados visuales
favorables, la ROP severa continúa como fuerte predictor de discapacidades no-visuales
independiente de injuria cerebral (7).
Dada esta conexión entre ROP severa y discapacidades no-visuales, nuestra hipótesis fue que ROP
severa podría estar asociada con retraso de la maduración de sustancia blanca en RNM avanzada.
La maduración de la sustancia blanca está bien reconocida como importante predictor de los
resultados de ND en infantes nacidos PT (8).
Los objetivos de este estudio de cohorte prospectivo de neonatos EPT fueron determina el
impacto de ROP severa en (1) desarrollo cerebral temprano medido por imagen de tensor de
difusión (ITD) y estadísticas espaciales de tracto (TBSS); y (2) resultados motores y cognitivos a los
18 meses de EC. Testeamos la hipótesis de que ROP severa estaría asociada con anormalidades
en el desarrollo temprano microestructural del cerebro, y con peor desarrollo cognitivo y motor
en el seguimiento a los 18 meses de EC.
MATERIAL Y MÉTODOS
Participantes
Este estudio fue aprobado por la Universidad de British Columbia / Children´s and Women´s
Health Centre of British Columbia Research Ethics Board. Como parte de un estudio prospectivo
más extenso de neonatos nacidos a 24-32 semanas de EG, se obtuvo consentimiento informado
de padres/cuidadores antes del reclutamiento de los RN desde Abril del 2006 a Abril del 2013 en
el BC Women´s Hospital (BCWH), el centro de referencia más grande de tercer nivel provincial.
Los RN fueron excluidos si tenían (1) evidencia clínica de malformación congénita o síndrome, (2)
infección congénita o (3) evidencia por ultrasonido de infarto hemorrágico parenquimatoso
extenso (>2 cm) (9). Esta cohorte ha sido descripta previamente (8, 10-13). Sólo los RN EPT nacidos
≤28 semanas de EG fueron incluidos en este sub-estudio ya que son el subgrupo con el mayor
riesgo de ROP severa.
Características clínicas
El tamizaje fue hecho por un oftalmólogo pediatra en BCWH según la Clasificación Internacional
de ROP, y se incluyó en el análisis la máxima severidad encontrada de ROP en los exámenes
secuenciales (14). ROP severa fue definida como ROP requiriendo tratamiento según el estudio
Tratamiento precoz de ROP (ETROP) (15). El tratamiento con anti- VEGF no estaba en uso en
nuestra institución al momento del estudio. Las características clínicas fueron recolectadas
sistemáticamente por revisión de las historias clínicas, como se describió previamente (11, 16):
DBP fue definido como oxigenoterapia más allá de las 36 semanas de edad postmenstrual (EPM),

hipotensión como cualquier tratamiento para baja presión sanguínea, infección con cultivo
positivo como cualquier cultivo positivo de sangre, orina, líquido CFR o respiratorio, y ECN según
criterios 2 y 3 de Bell (17).
RNM
Los neonatos fueron scaneados por primera vez cuando estuvieron clínicamente estables en el
período pretérmino y luego en la edad equivalente al término. Los estudios fueron todos
completados sin sedación farmacológica en un equipo Siemens 1.5 Tesla Avanto con imágenes
tridimensionales potenciadas en T1 volumétrica coronal e imágenes eco del espín rápido axiales
potenciadas en T2 realizadas en ambos momentos. Los RNs fueron escaneados usando un equipo
RNM compatible con incubadora (Lammers Medical Technology, Luebeck, Germany) y una bobina
de cabeza especial neonatal (Advanced Imaging Research, Cleveland, Ohio, USA). Un neuro-
radiólogo experimentado, ciego al historial médico del participante, revisó las imágenes y registró
la severidad de la injuria de la sustancia blanca (ISB), hemorragia intraventricular (HIV),
ventriculomegalia y hemorragia cerebelosa de acurdo a escalas previamente descriptas en esta
cohorte (11, 18). El score de mayor severidad de injuria visto entre el scan de pretérmino o término
fue empleado para los resultados del análisis de RNM dado que la severidad creciente tendría el
mayor impacto sobre los resultados del desarrollo.
Imagen de tensor de difusión
DTI refleja la difusión del agua en una elipse con difusión axial (λ1), el movimiento preferido del
agua a lo largo de los tractos de sustancia blanca, y difusión radial (λ2 y λ3) reflejando los planos
opuestos. DTI caracteriza la distribución espacial 3D de la difusión de agua en cada vóxel de la
RNM, proveyendo una medida indirecta del desarrollo microestructural (19-21). La AF, el
promedio de la direccionalidad de la difusión, aumenta con la maduración de la sustancia blanca,
reflejando la maduración de la línea celular de oligodendrocitos y eventos tempranos de
mielinización (20, 22). Los parámetros DTI de AF, λ1, λ2 y λ3 fueron medidos en siete regiones de
interés (ROI) de la sustancia blanca ubicadas manualmente y adquiridos empleando una secuencia
plana de eco de multirepetición de disparo simple (11). ROIs fueron ubicados por un neurólogo
experimentado cegado a la historia clínica y excluído si se presentaban significativos artefactos
de movimiento. Los ROIs fueron tomados en regiones anatómicas de calcarina, anterior, central y
posterior de la sustancia blanca, radiaciones ópticas, splenium del cuerpo calloso, y extremidad
posterior de la cápsula interna (PLIC), y fueron analizados utilizando un tiempo de interacción
entre los dos escaneos para caracterizar los cambios madurativos. Se ha mostrado previamente
que estas regiones se correlacionan con los resultados motor, de lenguaje y cognitivo (8-11).

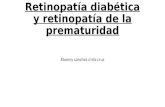
Figura 1 Valores de anisotropía fraccional media (AF) en aquellos con y sin ROP severa según edad postmenstrual del
scan en (A) sustancia blanca posterior (p<0.05) y (B) radiaciones ópticas (p<0.10). Mapa modelo de región de interés en
Imagen de tensor de difusión(C) al nivel del centro semioval alto y (D) al nivel de los ganglios basales. AWM, sustancia
Radiaciones Ópticas
ROP severa NO Rop severa
ROP severa NO Rop severa
ROP severa NO Rop severa
ROP severa NO Rop severa
Sustancia blanca posterior
Edad Edad

blanca anterior; CCWM, sustancia blanca calcarina; CWM, sustancia blanca central; OR, radiaciones ópticas; PLIC,
extremo posterior de la cápsula interna; PWM, sustancia blanca posterior; SCC, esplenio del cuerpo calloso.
TBSS, una evaluación semi-automática de AF por medio de tractos de sustancia blanca,
provee una medida menos usuario-dependiente de AF que los análisis complementarios
basados en ROI. TBSS fue desarrollada usando RNM funcional de la FSL, y después de
corrección por corrientes de Foucault cada volumen DTI fue registrado en un volumen
no- DTI para cada sujeto (23). Los datos AF TBSS fueron proyectados en un esqueleto
de AF media, que fue empleado para aplicar la estadística voxel de sujeto cruzado (23).
Utilizamos cinco plantillas basadas en la edad y pudimos comparar los grupos de
neonatos con un análisis estandarizado y un cálculo de umbral de significancia voxel de
p<0.05 ajustado por EPM al momento del scan (12). Las anormalidades de la sustancia
blanca detectadas con TBSS en la edad equivalente al término han mostrado predecir los
resultados del neurodesarrollo en neonatos prematuros (12, 24).
Seguimiento del desarrollo
A los 18 meses de EC, el ND fue evaluado con la escala Bayley-III, scores cognitivo,
lenguaje, y motor con una media de 100 y DS de 15 (25). Los evaluadores fueron
terapistas calificados cegados a los hallazgos de las imágenes de los participantes.
Parálisis cerebral severa fue definida como aquella diagnosticada por un clínico
experimentado en la evaluación de los 18 meses. El déficit auditivo se diagnosticó cuando
los audiogramas mostraron un umbral de audición >70 dB. La agudeza visual fue
determinada secuencialmente por el oftalmólogo tratante usando una variedad de
técnicas de evaluación dependiendo de la edad en el seguimiento y se obtuvieron con
una revisión retrospectiva de la historia clínica. Déficit visual fue definido ante mejor
agudeza visual <20/100. El estado socioeconómico fue determinado como el número de
años de educación materna.
Análisis de datos
El análisis estadístico se realizó empleando Stata V.14.1 (26). Las características clínicas
fueron comparadas empleando el test exacto de Fisher y el de Kruskal- Wallis para datos
categóricos y continuos, respectivamente, con una significancia estadística de p<0.05. La
asociación de ROP severa y otras variables clínicas con RNM fue testeada con regresión
logística univariada. Los valores medios de AF, promediados bilateralmente, fueron
comparados entre neonatos con y sin ROP severa, en un modelo generalizado de
regresión por mínimos cuadrados para medidas repetidas, ajustando por EPM en RNM
y múltiples ROIs con p<0.05. Examinamos la relación de ROP con AF modificada por EPM
en el scan RNM, considerando una interacción de p<0.1 como significativa.
RESULTADOS
Características clínicas
De 234 neonatos nacidos a las 24-32 semanas de EG, 126 nacieron a las 24-28 semanas
de EG. Noventa y ocho (79%) neonatos extremadamente prematuros fueron evaluados
para ROP en el BCWH y fueron incluídos en el análisis; los infantes no evaluados fueron
mayores al nacer pero no hubo otras diferencias demográficas. Los RN tenían una

mediana de EG de 26.0 semanas (RIQ, 25.0-26.9 semanas). Los scans RNM tempranos se
completaron en 98 neonatos evaluados por ROP a una mediana de 32.4 semanas (RIQ,
30.3- 35.0 semanas), y la RNM equivalente al término fue realizada en 87 (89%) a una
mediana de EPC de 39.8 semanas (RIQ, 38.3-41.6 semanas).
Figura 2 TBSS empleando plantillas automáticas de neonatos de término y pretérmino. Las regiones de sustancia blanca
donde los RN con ROP severa difieren de aquellos sin ROP severa (p<0.05), EC al scan, mostraron un lecho azul en el
esqueleto de sustancia blanca en amarillo. AF, anisotropía fraccional; EG, edad gestacional.
Retinopatía de la prematurez
De los 98 neonatos en esta cohorte, 67 (68%) presentaron algún estadío de ROP (estadio
1=7, estadio 2=47, estadío 3=13, estadío 4=0, estadío 5=0), y 19 (19%) requirieron
tratamiento por ROP severa según los criterios definidos en el estudio ETROP a una EPM
mediana de 37.9 semanas (RIQ, 36.1-39.3 semanas).No hubo diferencias en los
parámetros clínicos o las tasas de injuria cerebral entre infantes sin ROP y aquellos con
ROP leve a moderada (estadíos 1 y 2) (todos p>0.05) Parámetros neonatales asociados
con ROP severa incluyeron EG al nacer, PN, talla al nacer, CC al nacer, DBP, ECN e
hipotensión (Tabla 1).
Injuria cerebral
Se clasificaron 98 scaneos tempranos y 87 a edad equivalente al término. Los hallazgos
incluyeron injurias de SB en 30(35%) neonatos, injuria severa de SB en 9 (11%), HIV en
47 (55%), HIV severa en 5 (6%), ventriculomegalia en 27 (32%) y hemorragia cerebelosa
en 16 (19%). ROP severa no estuvo asociada con riesgo aumentado de injuria de SB, HIV,
ventriculomegalia o hemorragia cerebelosa aún al comparar las formas más severamente
afectadas de injuria SB, HIV y ventriculomegalia separadamente (p>0.05) (tabla 1).
Término 42 + sem EG
Pretérmino 34-37 sem EG
Leyenda Regiones de sustancia blanca con ROP severa (p<0.05) Esqueleto en AF de sustancia blanca

Maduración de la sustancia blanca
La AF media en neonatos con ROP severa fue significativamente menor para la sustancia
blanca posterior (efecto de tamaño, -0.024; IC 95% -0.044 a -0.004; p=0.018) con una
significativa interacción en el tiempo (p=0.078) (figura 1). La AF de las radiaciones ópticas
(efecto de tamaño, -0.019; IC 95% -0.39 a 0.001; p=0.066) (figura 1) fue no significativa
en el análisis no ajustado. Empleando el análisis de regresión voxel en TBSS, las regiones
de sustancia blanca con AF significativamente más baja en ROP severa incluyeron las
radiaciones ópticas, PLIC y cápsula externa en los scans de las 34-37 semanas (n=30) y
42+ semanas de EG (n=24) (figura 2). La AF en el análisis ROI de la sustancia blanca
anterior (efecto de tamaño, 0.001; p=0.930), sustancia blanca central (efecto de tamaño,
-0.002; p=0.842), esplenio del cuerpo calloso (efecto de tamaño, -0.010; p=0.499), PLIC
(efecto de tamaño, -0.014; p=0.193) y sustancia blanca calcarina (efecto de tamaño, -
0.002; p=0.778) no difirieron significativamente en neonatos con y sin ROP. En la
sustancia blanca posterior y radiaciones ópticas, hubo una relación similar con ROP
severa en los ejes de difusión radial (λ2 y λ3) y axial (λ1).
Resultados del desarrollo
Un total de 83 (85%) infantes fueron examinados en seguimiento a los 18 meses de EC
(Tabla 2); no hubo diferencias significativas en los siete que se apartaron del estudio
después de al menos una RNM o los ocho que abandonaron el seguimiento.
Los infantes con ROP severa tuvieron scores más bajos cognitivos y motor en Bayley III,
sin diferencias en el score de lenguaje en relación a infantes sin ROP severa. No hubo
diferencias en los años de educación materna entre grupos (p=0.907). En el modelo
multivariado, la relación entre ROP severa y los scores motor y cognitivo permaneció
significante al ajustar por EG al nacer e injuria severa de SB y/o HIV (tabla 3).
Un infante en el grupo de ROP no severo no pudo completar la evaluación de Bayley-III
debido a PC severa y déficit visual cortical; cuando se asignó un valor de 2 DS por debajo
de la media, no hubo diferencia significativa en los hallazgos. No hubo diferencia en la
tasa de PC, déficit auditivo o visual en infantes con y sin ROP severa (tabla 2). Los
exámenes de agudeza visual no fueron hechos sistemáticamente, pero estuvieron
disponibles para la revisión de la historia clínica en 12 (63%) RN con ROP severa a una
edad media de 3.9 años (RIQ, 3.1-5.0 años). La agudeza visual media fue 20/30 dioptrías
(ojo derecho) y 20/40 dioptrías (ojo izquierdo) en infantes con ROP; ningún infante
cumplió los criterios de severo déficit visual.

DISCUSIÓN
En una cohorte prospectiva longitudinal de neonatos extremadamente prematuros,
encontramos una demora significativa en la maduración de las regiones de la sustancia
blanca posterior en el análisis de TBSS de las radiaciones ópticas, PLIC y cápsula externa
en aquellos RN con ROP severa. Estos novedosos hallazgos ocurrieron
independientemente de injuria severa a de SB o HIV y posiblemente indiquen
mecanismos vitales similares en el desarrollo de ROP severa con pobre maduración de
la sustancia blanca. Nuestro estudio también enfatiza cómo los resultados adversos
motor y cognitivo están asociados con retrasos madurativos en ITD y TBSS
independientes de los marcadores tradicionales de injuria cerebral en el neonato
pretérmino.
VEGF es importante en el desarrollo de ROP severa, con una terapia anti-VEGF
actualmente aprobada para ROP severa. Los niveles circulantes factor de crecimiento 1
insulina-símil (IGF-1) son conocidos como un importante factor de cambio de los niveles

circulantes de VEGF. Dentro del cerebro, IGF-1 ha mostrado tener un rol significante en
el aumento y utilización de glucosa a través de todas las líneas celulares neurales (6, 27,
28). Las concentraciones medias de IGF-1 entre el nacimiento y las 35 semanas de EPM
en neonatos prematuros han mostrado correlación con los volúmenes del cerebro total,
sustancia blanca, sustancia gris y cerebeloso, con desarrollo más pobre en aquellos niños
con tasa de aumento más lenta (29, 30). Estos datos apoyan que los potenciales
mediadores de ROP severa son marcadores de desarrollo cerebral adverso,
independientemente de los resultados visuales, y están resaltados por nuestras
evaluaciones del seguimiento a los 18 meses de EC mostrando scores más bajos
cognitivo y motor en aquellos con ROP severa, consistente con cohortes más amplias (3,
4, 31). Mientras que ROP severa estuvo menos fuertemente relacionada con el resultado
en lenguaje, esto puede reflejar la robustez limitada de la evaluación de lenguaje a los
18 meses de EC.
El retraso de maduración de las radiaciones ópticas es consistente con estudios previos
empleando ITD y TBSS en neonatos prematuros que mostraron una relación entre ROP
severa y desarrollo microestructural demorado de la sustancia blanca en las radiaciones
ópticas en la edad equivalente al término, independiente de la injuria de sustancia blanca
(32, 33). Investigaciones a los 7 años de edad mostraron demora en la microestructura
de las radiaciones ópticas en niños con historia de ROP severa comparados con aquellos
con ROP más leve (32). Hemos mostrado que estas demoras están presentes en el
período de pretérmino tardío, y comprometen vías no-visuales, señalando el nexo
temprano de la ROP severa con pobre maduración de la sustancia blanca en neonatos
prematuros.
El grosor de la capa fibrosa del nervio retinal (RNFL), determinada con tomografía óptica,
ha mostrado ser inversamente proporcional con el estadío de ROP, con mayor
compromiso en la ROP severa (34). Considerando una relación entre la maduración de la
sustancia blanca y el desarrollo retiniano, investigación previa ha mostrado que menor
grosor de RNFL a través del manojo maculopapular se correlacionó con scores del
desarrollo motor y cognitivo más bajos a los 18 y 24 meses de EC (35). Estos hallazgos
proveen una mirada dentro de las asociaciones entre la retina y las vías de sustancia
blanca subyacentes, y ofrecen una “ventana hacia el cerebro de las conexiones que los
gangliones retinianos y células foto receptoras comparten con las vías de la sustancia
blanca. Las demoras en la maduración de las vías motora, visual y asociación visual del
cerebro en desarrollo detectadas en neonatos con ROP severa sugieren un mecanismo
por el cual estos factores pueden actuar sobre el neurodesarrollo.
Limitaciones
Pese a que pudimos comparar un gran número de RN EPT con RNM seriadas, la
oportunidad de los scans RNM en el seguimiento pueden haber afectado los resultados
de las imágenes debido al desarrollo de ROP en el tiempo como un desorden adquirido
progresivamente. No pudimos controlar la oportunidad de la terapia láser en retina con
ROP y su posible impacto sobre los hallazgos en la imagen del cerebro. El seguimiento
de la agudeza visual no estuvo estandarizado en la cohorte o realizado en conjunción
con los exámenes del ND a los 18 meses de EC.
CONCLUSIONES

La ROP severa que requiere tratamiento con fotocoagulación láser está asociada con
demora de la maduración en las vías motoras, visual y de asociación visual. ROP severa
predijo menor funcionamiento motor y cognitivo a los 18 meses de EC, independiente
de injuria cerebral severa y EG al nacer. Mayor investigación es necesaria para determinar
qué mecanismos potenciales en la ROP severa evitan el ND óptimo y para determinar los
impactos del tratamiento temprano y efectivo de la ROP severa en la maduración del
cerebro.
REFERENCIAS
1 Lee J, Dammann O. Perinatal infection, inflammation, and retinopathy of prematurity. Semin
Fetal Neonatal Med 2012;17:26–9.
2 Gunther JB, Altaweel MM. Bevacizumab (Avastin) for the treatment of ocular disease. Surv
Ophthalmol 2009;54:372–400.
3 Schmidt B, Asztalos EV, Roberts RS, et al. Impact of bronchopulmonary dysplasia, brain injury,
and severe retinopathy on the outcome of extremely low-birth-weight infants at 18 months:
results from the trial of indomethacin prophylaxis in preterms. JAMA 2003;289:1124–9.
4 Bassler D, Stoll BJ, Schmidt B, et al. Using a count of neonatal morbidities to predict poor
outcome in extremely low birth weight infants: added role of neonatal infection. Pediatrics
2009;123:313–8.
5 Hellström A, Smith LE, Dammann O. Retinopathy of prematurity. Lancet 2013;382:1445–57.
6 Harrell SN, Brandon DH. Retinopathy of prematurity: the disease process, classifications,
screening, treatment, and outcomes. Neonatal Netw 2007;26:371–8.
7 Schmidt B, Davis PG, Asztalos EV, et al. Association between severe retinopathy of prematurity
and nonvisual disabilities at age 5 years. JAMA 2014;311:523–4.
8 Chau V, Synnes A, Grunau RE, et al. Abnormal brain maturation in preterm neonates associated
with adverse developmental outcomes. Neurology 2013;81:2082–9.
9 Papile LA, Burstein J, Burstein R, et al. Incidence and evolution of subependymal and
intraventricular hemorrhage: a study of infants with birth weights less than 1,500 gm. J Pediatr
1978;92:529–34.
10 Adams E, Chau V, Poskitt KJ, et al. Tractography-based quantitation of corticospinal tract
development in premature newborns. J Pediatr 2010;156:882–8.
11 Chau V, Poskitt KJ, McFadden DE, et al. Effect of chorioamnionitis on brain development and
injury in premature newborns. Ann Neurol 2009;66:155–64.
12 Duerden EG, Foong J, Chau V, et al. Tract-based spatial statistics in preterm-born neonates
predicts cognitive and motor outcomes at 18 months. AJNR Am J Neuroradiol 2015;36:1565–71.
13 Brummelte S, Grunau RE, Chau V, et al. Procedural pain and brain development in premature
newborns. Ann Neurol 2012;71:385–96.
14 International Committee for the Classification of Retinopathy of Prematurity. The international
classification of retinopathy of prematurity revisited. Arch Ophthalmol 2005;123:991–9.
15 Early treatment of retinopathy of prematurity cooperative group. Revised indications for the
treatment of retinopathy of prematurity. Arch Ophthalmol 2003;121:1684–96.
16 Chau V, Brant R, Poskitt KJ, et al. Postnatal infection is associated with widespread abnormalities
of brain development in premature newborns. Pediatr Res 2012;71:274–9.
17 Bell M, Ternberg J, Feigin R, et al. Therapeutic decisions based upon clinical staging. Annals of
Surgery 1978;187:1–7.
18 Miller SP, Ferriero DM, Leonard C, et al. Early brain injury in premature newborns detected with
magnetic resonance imaging is associated with adverse early neurodevelopmental outcome. J
Pediatr 2005;147:609–16.

19 Mukherjee P, Miller JH, Shimony JS, et al. Diffusion-tensor MR imaging of gray and white matter
development during normal human brain maturation. AJNR Am J Neuroradiol 2002;23:1445–56.
20 Miller SP, Vigneron DB, Henry RG, et al. Serial quantitative diffusion tensor MRI of the
premature brain: development in newborns with and without injury. J Magn Reson
Imaging 2002;16:621–32.
21 Beaulieu C. The basis of anisotropic water diffusion in the nervous system - a technical
review. NMR Biomed 2002;15:435–55.
22 Drobyshevsky A, Song SK, Gamkrelidze G, et al. Developmental changes in diffusion anisotropy
coincide with immature oligodendrocyte progression and maturation of compound action
potential. J Neurosci 2005;25:5988–97.
23 Smith SM, Jenkinson M, Johansen-Berg H, et al. Tract-based spatial statistics: voxelwise analysis
of multi-subject diffusion data. Neuroimage 2006;31:1487–505.
24 Counsell SJ, Maalouf EF, Fletcher AM, et al. MR imaging assessment of myelination in the very
preterm brain. AJNR Am J Neuroradiol 2002;23:872–81.
25 Bayley N. The bayley scales of infant development III. New York, New York: Psychological
Corporation, 2005.
26 StataCorp. Stata statistical software. Release 14 2015. College Station, TX: StataCorp LP.
27 Cheng CM, Reinhardt RR, Lee WH, et al. Insulin-like growth factor 1 regulates developing brain
glucose metabolism. Proc Natl Acad Sci U S A 2000;97:10236–41.
28 Joseph D’Ercole A, Ye P. Expanding the mind: insulin-like growth factor I and brain
development. Endocrinology 2008;149:5958–62.
29 Hansen-Pupp I, Hövel H, Hellström A, et al. Postnatal decrease in circulating insulinlike growth
factor-I and low brain volumes in very preterm infants. J Clin Endocrinol Metab 2011;96:1129–35.
30 Hansen-Pupp I, Holger H, Lofqvist C, et al. Circulatory IGF1 and brain volumes with
neurodevelopment in preterm infants. Pediatr Res 2013;74:564–9.
31 Schmidt B, Roberts RS, Davis PG, et al; Caffeine for Apnea of Prematurity (CAP) Trial
Investigators Caffeine for Apnea of Prematurity CAP Trial Investigators. Prediction of late death or
disability at age 5 years using a count of 3 neonatal morbidities in very low birth weight infants. J
Pediatr 2015;167:982–6.
32 Thompson DK, Thai D, Kelly CE, et al. Alterations in the optic radiations of very preterm
children-perinatal predictors and relationships with visual outcomes. Neuroimage Clin
2014;4:145–53.
33 Bassi L, Ricci D, Volzone A, et al. Probabilistic diffusion tractography of the optic radiations and
visual function in preterm infants at term equivalent age. Brain 2008;131:573–82.
34 Park KA, Oh SY. Retinal nerve fiber layer thickness in prematurity is correlated with stage of
retinopathy of prematurity. Eye 2015;29:1594–602.
35 Rothman AL, Sevilla MB, Mangalesh S, et al. Thinner retinal nerve fiber layer in very preterm
versus term infants and relationship to brain anatomy and neurodevelopment. Am J Ophthalmol
2015;160:1296–308.

F532 Glass TJA, et al. Arch Dis Child Fetal Neonatal Ed 2017;102:F532–F537. doi:10.1136/archdischild-2016-312533
AbstrActObjective To determine whether severe retinopathy of prematurity (ROP) is associated with (1) abnormal white matter maturation and (2) neurodevelopmental outcomes at 18 months’ corrected age (CA) compared with neonates without severe ROP.Design We conducted a prospective longitudinal cohort of extremely preterm neonates born 24–28 weeks’ gestational age recruited between 2006 and 2013 with brain MRIs obtained both early in life and at term-equivalent age. Severe ROP was defined as ROP treated with retinal laser photocoagulation. Using diffusion tensor imaging and tract-based spatial statistics (TBSS), white matter maturation was assessed by mean fractional anisotropy (FA) in seven predefined regions of interest. Neurodevelopmental outcomes were assessed with Bayley Scales of Infant and Toddler Development-III (Bayley-III) composite scores at 18 months’ CA. Subjects were compared using Fisher’s exact, Kruskal-Wallis and generalised estimating equations.setting Families were recruited from the neonatal intensive care unit at BC Women’s Hospital.Patients Of 98 extremely preterm neonates (median: 26.0 weeks) assessed locally for ROP, 19 (19%) had severe ROP and 83 (85%) were assessed at 18 months’ CA.results Severe ROP was associated with lower FA in the posterior white matter, and with decreased measures of brain maturation in the optic radiations, posterior limb of the internal capsule (PLIC) and external capsule on TBSS. Bayley-III cognitive and motor scores were lower in infants with severe ROP.conclusions Severe ROP is associated with maturational delay in the optic radiations, PLIC, external capsule and posterior white matter, housing the primary visual and motor pathways, and is associated with poorer cognitive and motor outcomes at 18 months’ CA.
IntrODuctIOnRetinopathy of prematurity (ROP) is a prolifera-tive disorder of retinal vascularisation that is most severe in extremely preterm neonates born at less than 28 weeks’ gestational age (GA). Primary ther-apeutic strategies for ROP include prevention of abnormal vessel development with tight control of supplemental oxygen therapy and, when severe, treatment with either retinal laser photocoagulation therapy or more recently intravitreal antivascular
endothelial growth factor (anti-VEGF).1 2 Several large cohort studies of preterm neonates have shown that severe ROP is associated with lower cognitive and motor scores in early childhood.3–6 Despite favourable visual outcomes, severe ROP continues to strongly predict non-visual disabilities independent of brain injury.7
Given this link between severe ROP and non-vi-sual disabilities, we hypothesised that severe ROP would be associated with white matter matura-tional delay on advanced MRI. White matter matu-ration is well recognised as an important predictor of neurodevelopmental outcomes in infants born preterm.8
The objectives of this prospective cohort study of extremely preterm neonates were to determine the impact of severe ROP on (1) early brain develop-ment as measured by MR diffusion tensor imaging (DTI) and tract-based spatial statistics (TBSS); and (2) motor and cognitive outcomes at 18 months’ corrected age (CA). We tested the hypothesis that severe ROP would be associated with abnormali-ties in early brain microstructural development, and with worse cognitive and motor development at 18 months’ CA follow-up.
What this study adds?
► Cognitive and motor developmental scores at 18 months’ corrected age were preferentially impacted in infants with severe ROP.
► White matter maturation in the posterior limb of the internal capsule, external capsule and optic radiations was delayed in infants with severe ROP.
Original article
Severe retinopathy of prematurity predicts delayed white matter maturation and poorer neurodevelopmentTorin J A Glass,1,2 Vann Chau,1,2,3 Jane Gardiner,3,4 Justin Foong,2 Jillian Vinall,5 Jill G Zwicker,3,6,7,8 Ruth E Grunau,3,9 Anne Synnes,3,9 Kenneth J Poskitt,3,10 Steven P Miller1,2,3
to cite: Glass TJA, Chau V, Gardiner J, et al. Arch Dis Child Fetal Neonatal Ed 2017;102:F532–F537.
For numbered affiliations see end of article.
correspondence to Steven P Miller, Department of Pediatrics (Neurology), University of Toronto and the Hospital for Sick Children, Toronto (Ontario) M5G 1X8, Canada; steven. miller@ sickkids. ca
Received 15 December 2016Revised 4 April 2017Accepted 6 April 2017Published Online First 23 May 2017
What is already known on this topic?
► Severe retinopathy of prematurity (ROP) is a potentially devastating retinal disorder of the preterm infant that can be treated with retinal photocoagulation therapy to preserve vision.
► Severe ROP is associated with poor neurodevelopmental outcomes despite favourable visual outcomes.
group.bmj.com on March 31, 2018 - Published by http://fn.bmj.com/Downloaded from

F533Glass TJA, et al. Arch Dis Child Fetal Neonatal Ed 2017;102:F532–F537. doi:10.1136/archdischild-2016-312533
table 1 Demographic, clinical characteristics and imaging findings of neonates 24–28 weeks’ GA with and without severe ROP treated with retinal laser therapy
no severe rOP (n=79) severe rOP (n=19) p Value
Male 38 (48%) 14 (74%) 0.072
Multiple gestation 5 (6%) 4 (21%) 0.068
Age at birth (weeks) 26.1 (25.3–27.1) 25.4 (24.7–25.9) 0.003
Weight at birth (g) 845 (745–991) 700 (630–795) <0.001
Length at birth (cm) 34 (32–36) 32 (31–34) 0.015
Head circumference at birth (cm) 24 (22.5–25) 22.5 (22–23) 0.005
Conventional ventilation (days) 16 (5–33) 51 (37–59) <0.001
Histological chorioamnionitis 39 (51%) 9 (53%) >0.999
Hypotension 37/79 (47%) 15/19 (79%) 0.020
Bronchopulmonary dysplasia 22/79 (28%) 11/19 (58%) 0.017
Necrotising enterocolitis 3/79 (4%) 4/19 (21%) 0.025
Culture positive infection 46/79 (58%) 15/19 (79%) 0.115
Intraventricular haemorrhage 43/78 (55%) 10/19 (53%) >0.999
White matter injury 24/78 (31%) 8/19 (42%) 0.417
Cerebellar haemorrhage 16/78 (21%) 2/19 (11%) 0.512
Severe WMI and/or IVH 12/78 (15%) 3/19 (16%) >0.999
Number (%) or median (IQR).GA, gestational age; IVH, intraventricular haemorrhage; ROP, retinopathy of prematurity; WMI, white matter injury.
Original article
MAterIAls AnD MethODsParticipantsThis study was approved by the University of British Columbia/Children’s and Women’s Health Centre of British Columbia Research Ethics Board. As part of a larger prospective study of neonates born 24–32 weeks’ GA, informed consent was obtained from parents/guardians prior to recruitment of the neonates from April 2006 to April 2013 at BC Women’s Hospital (BCWH), the major provincial tertiary-level neonatal referral centre. Neonates were excluded if they had (1) clinical evidence of a congenital malformation or syndrome, (2) congenital infection or (3) ultra-sound evidence of a large parenchymal haemorrhagic infarction (>2 cm).9 This cohort has been described previously.8 10–13 Only extremely preterm neonates born ≤28 weeks’ GA were included in this substudy as they are the subset at greatest risk of severe ROP.
clinical characteristicsNeonates were screened by a paediatric ophthalmologist at BCWH as per the International Classification of Retinopathy of Prematurity, and the maximal ROP severity in sequential assessments was included in the analysis.14 Severe ROP was defined as ROP requiring treatment as per the Early Treat-ment for Retinopathy of Prematurity (ETROP) study.15 Intra-vitreal anti-VEGF treatment was not used at our institution at the time of the study. Clinical characteristics were collected systematically by chart review, as described previously11 16: bronchopulmonary dysplasia (BPD) was defined as oxygen therapy beyond 36 weeks’ postmenstrual age (PMA), hypo-tension as any treatment for low blood pressure, culture posi-tive infection as any positive blood, urine, cerebrospinal fluid or respiratory culture, and necrotising enterocolitis (NEC) as stages 2 and 3 of Bell’s criteria.17
MrI studiesNeonates were scanned first when clinically stable in the preterm period and again at term-equivalent age. MRI studies were all completed without pharmacological sedation on a Siemens 1.5 Tesla Avanto scanner with three-dimensional (3D)
coronal volumetric T1-weighted and axial fast-spin echo T2-weighted images performed at both time-points. Neonates were scanned using an MRI-compatible isolette (Lammers Medical Technology, Luebeck, Germany) and specialised neonatal head coil (Advanced Imaging Research, Cleveland, Ohio, USA). An experienced neuroradiologist, blinded to the participant’s medical history, reviewed the images and recorded the white matter injury severity (WMI), intraven-tricular haemorrhage (IVH), ventriculomegaly and cerebellar haemorrhage according to scales previously described in this cohort.11 18 The most severe injury severity score seen between the preterm or term scan was used in the MRI analysis results as increasing severity would have the greatest impact on devel-opmental outcomes.
Diffusion tensor imagingDTI reflects the water diffusion in an ellipsoid space with axial diffusion (λ1), the preferred movement of water along the white matter tracts, and radial diffusion (λ2 and λ3) reflecting the opposite planes. DTI characterises the 3D spatial distribu-tion of water diffusion in each voxel of the MRI, providing an indirect measure of microstructural development.19–21 Fractional anisotropy (FA), the average directionality of diffu-sion, increases with white matter maturation, reflecting the maturation of the oligodendrocyte lineage and early events of myelination.20 22 DTI parameters of FA, λ1, λ2 and λ3 were measured in seven manually placed white matter regions of interest (ROI) and acquired using a multirepetition single-shot echo planar sequence.11 ROIs were placed by an experienced neurologist blinded to the clinical history and excluded if signif-icant motion artefact was present. The ROIs were acquired in the anatomical regions of the calcarine, anterior, central and posterior white matter regions, optic radiations, splenium of the corpus callosum, and posterior limb of the internal capsule (PLIC), and were analysed using a time interaction between the two scans to characterise the maturational changes. These regions have been shown previously to correlate with motor, language and cognitive outcomes.8 11
group.bmj.com on March 31, 2018 - Published by http://fn.bmj.com/Downloaded from

F534 Glass TJA, et al. Arch Dis Child Fetal Neonatal Ed 2017;102:F532–F537. doi:10.1136/archdischild-2016-312533
Figure 1 Mean fractional anisotropy (FA) values in those with and without severe retinopathy of prematurity (ROP) by postmenstrual age at scan in (A) posterior white matter (p<0.05) and (B) optic radiations (p<0.10). Diffusion tensor imaging region of interest model map (C) at the level of the high centrum semiovale and (D) at the level of the basal ganglia. AWM, anterior white matter; CCWM, calcarine white matter; CWM, central white matter; OR, optic radiations; PLIC, posterior limb of the internal capsule; PWM, posterior white matter; SCC, splenium of the corpus callosum.
Original article
TBSS, a semi-automated assessment of FA across white matter tracts, provides a less user-dependent measure of FA than complementary ROI-based analyses. TBSS was performed using functional MRI of the brain software library (FSL), and after correction for eddy currents each DTI volume was registered to a non-DTI volume for each subject.23 The TBSS FA data were projected onto a mean FA tract skeleton, which was used to apply the voxelwise cross-subject statis-tics.23 We used five age-based templates and were able to compare neonate groups with a standardised analysis and a calculated voxel significance threshold of p<0.05 adjusted for PMA at scan.12 White matter abnormalities detected with TBSS at term-equivalent age have been shown to predict neurodevelopmental outcomes in preterm neonates.12 24
Developmental follow-upAt 18 months’ CA, neurodevelopment was assessed with the Bayley Scales of Infant and Toddler Development-III (Bayley-III)
cognitive, language and motor composite scores with a mean of 100 and SD of 15.25 Assessors were qualified therapists blinded to the imaging findings of the participants. Severe cerebral palsy was defined as that which was diagnosed by an experienced clinician by the 18-month assessment. Hearing impairment was diagnosed when audiograms showed hearing threshold >70 dB. Visual acuity was assessed sequentially by the treating ophthal-mologist using varied assessment techniques depending on age at follow-up and collected with a retrospective chart review. Visual impairment was defined as best visual acuity <20/200. Socio-economic status was assessed as number of years of maternal education.
Data analysisStatistical analysis was performed using Stata V.14.1.26 Clin-ical characteristics were compared using Fisher’s exact and the Kruskal-Wallis tests for categorical and continuous data, respec-tively, with a statistical significance of p<0.05. The association
group.bmj.com on March 31, 2018 - Published by http://fn.bmj.com/Downloaded from

F535Glass TJA, et al. Arch Dis Child Fetal Neonatal Ed 2017;102:F532–F537. doi:10.1136/archdischild-2016-312533
Figure 2 Tract-based spatial statistics (TBSS) using automated preterm and term neonate templates. White matter regions where neonates with severe retinopathy of prematurity (ROP) differ from those with no severe ROP (p<0.05), corrected for age at scan, shown in blue overlaid on the white matter skeleton in yellow. FA, fractional anisotropy; GA, gestational age.
table 2 18-month corrected age (CA) follow-up assessments of neonates 24–28 weeks’ GA with and without severe ROP treated with retinal laser therapy
no severe rOP (n=67) severe rOP (n=16) p Value
Bayley-III cognitive score 105 (100–115) 95 (88–105) 0.016
Bayley-III motor score 94 (85–110) 85 (75–93) 0.012
Bayley-III language score 96 (83–112) 89 (83–103) 0.321
Severe cerebral palsy 6/67 (9%) 1/16 (6%) >0.999
Visual impairment 1/67 (1%) 0/16 (0%) >0.999
Hearing impairment 2/67 (3%) 0/16 (0%) >0.999
Number (%) or median (IQR).Bayley-III, Bayley Scales of Infant and Toddler Development-III; GA, gestational age; ROP, retinopathy of prematurity.
table 3 Multivariate linear regression analysis of the association between severe retinopathy of prematurity and each of the 18-month corrected age Bayley composite scores adjusted for gestational age at birth and severe white matter injury and/or intraventricular haemorrhage
effect size (95% cI) p Value
Bayley-III cognitive composite −9.22 (−17.69 to −0.75) 0.033
Bayley-III motor composite −10.77 (−19.87 to −1.66) 0.021
Bayley-III language composite −3.45 (−13.80 to 6.89) 0.508
Bayley-III, Bayley Scales of Infant and Toddler Development-III.
Original article
of severe ROP and other clinical variables with WMI was tested with univariate logistic regression. The mean values of FA, aver-aged bilaterally, were compared between neonates with and without severe ROP, in a generalised least squares regression model for repeated measures, adjusting for PMA at MRI scan and multiple ROIs with a p<0.05. We examined the relationship of ROP with FA modified by PMA at MRI scan, considering an interaction term p<0.1 as significant.
resultsclinical characteristicsOf the 234 neonates born 24–32 weeks’ GA, 126 were born at 24–28 weeks’ GA. Ninety-eight (79%) extremely preterm neonates were assessed for ROP at BCWH and were included in the analysis; infants not assessed were older at birth but had no difference in other demographics. Neonates were born at a median GA of 26.0 weeks (IQR, 25.0–26.9 weeks). Early MRI scans were completed in the 98 neonates assessed for ROP at a median of 32.4 weeks (IQR, 30.3–35.0 weeks), and term-equivalent MRI was performed in 87 (89%) at a median PMA of 39.8 weeks (IQR, 38.3–41.6 weeks).
retinopathy of prematurityOf the 98 neonates in this cohort, 67 (68%) had any stage of ROP (stage 1=7, stage 2=47, stage 3=13, stage 4=0 stage 5=0), and 19 (19%) neonates required treatment for severe ROP as per the criteria defined in the ETROP study at a median PMA of 37.9 weeks (IQR, 36.1–39.3 weeks). There was no difference
in the clinical parameters or brain injury rates between infants without ROP and those with mild to moderate ROP (stages 1 and 2) (all p>0.05). Neonatal parameters associated with severe ROP included GA at birth, birth weight, birth length, head circumference at birth, BPD, NEC and hypotension (table 1).
brain injuryNinety-eight early and 87 term-equivalent scans were scored. Findings included WMI in 30 (35%) neonates, severe WMI in 9 (11%), IVH in 47 (55%), severe IVH in 5 (6%), ventricu-lomegaly in 27 (32%) and cerebellar haemorrhage in 16 (19%). Severe ROP was not associated with an increased risk of WMI, IVH, ventriculomegaly or cerebellar haemorrhage even when comparing the most severely affected forms of WMI, IVH and ventriculomegaly separately (all p>0.05) (table 1).
White matter maturationMean FA in neonates with severe ROP was significantly lower for the posterior white matter (effect size, −0.024; 95% CI −0.044 to −0.004; p=0.018) with a significant interaction over time (p=0.078) (figure 1). The FA of the optic radiations (effect size, −0.019; 95% CI −0.39 to 0.001; p=0.066) (figure 1) was not significant on unadjusted analysis. Using voxelwise regres-sion analysis in TBSS, white matter regions with significantly lower FA in severe ROP included the optic radiations, PLIC and external capsule on scans at 34–37 weeks (n=30) and 42+ weeks’ GA (n=24) (figure 2). FA on ROI analysis in the anterior white matter (effect size, 0.001; p=0.930), central white matter (effect size, −0.002; p=0.842), splenium of the corpus callosum (effect size, −0.010; p=0.499), PLIC (effect size, −0.014; p=0.193) and calcarine white matter (effect size, −0.002; p=0.778) did not differ significantly in neonates with and without ROP. In the posterior white matter and optic radiations, there was a similar relationship with severe ROP in the radial (λ2 and λ3) and axial (λ1) diffusion axes.
Developmental outcomesA total of 83 (85%) infants were assessed at 18 months’ CA follow-up (table 2); there were no significant differences in the seven who withdrew from the study after at least one MRI scan or the eight who were lost to follow-up.
Infants with severe ROP had lower Bayley-III motor and cognitive scores, with no difference in language scoring relative to infants without severe ROP. There was no difference in years of maternal education between groups (p=0.907). In a multivar-iate model, the relationship between severe ROP and motor and cognitive scores remained significant when adjusting for GA at birth and severe WMI and/or IVH (table 3).
One infant in the no severe ROP group was unable to complete the Bayley-III assessment due to severe cerebral palsy and cortical visual impairment; when assigned a value of 2 SD below
group.bmj.com on March 31, 2018 - Published by http://fn.bmj.com/Downloaded from

F536 Glass TJA, et al. Arch Dis Child Fetal Neonatal Ed 2017;102:F532–F537. doi:10.1136/archdischild-2016-312533
Original article
the mean, there was no meaningful difference in the findings. There was no difference in the rate of cerebral palsy, hearing or visual impairment in infants with and without severe ROP (table 2). Visual acuity assessments were not done systematically, but were available on chart review in 12 (63%) newborns with severe ROP at a median age of 3.9 years (IQR, 3.1–5.0 years). Median visual acuity was 20/30 OD (right eye) and 20/40 OS (left eye) in infants with ROP; no infants met the guidelines for severe visual impairment.
DIscussIOnIn a prospective longitudinal cohort of extremely premature neonates, we found a significant maturational delay of the poste-rior white matter regions with delay on TBSS analysis in the optic radiations, PLIC and external capsule in those neonates with severe ROP. These novel findings occurred independent of severe white matter injury or intraventricular haemorrhage and likely indicate similar vital mechanisms in the development of severe ROP with poor maturation of the white matter. Our study also emphasises how adverse motor and cognitive develop-mental outcomes are associated with maturational delays on DTI and TBSS independent of the traditional markers of brain injury in the preterm neonate.
VEGF is important in the development of severe ROP, with an anti-VEGF therapy currently approved for severe ROP. Circu-lating levels of insulin-growth factor 1 (IGF-1) are known to be an important modifier in the circulatory levels of VEGF. Within the brain, IGF-1 has been shown to have a significant role in the augmentation and utilisation of glucose across all neural cell lineages.6 27 28 Mean IGF-1 concentrations between birth and 35 weeks’ PMA in preterm neonates have been shown to correlate with total brain, white matter, grey matter and cere-bellar brain volumes, with poorer cognitive development seen in those infants with the slowest rate of increase.29 30 These data support potential mediators of severe ROP as markers of adverse brain development, independent of visual outcomes, and are highlighted by our 18-month CA follow-up assessments showing lower cognitive and motor developmental scores in those with severe ROP, consistent with larger cohorts.3 4 31 While severe ROP was less strongly related to language outcome, this may reflect the limited robustness of language assessment at 18 months’ CA.
Maturational delays in the optic radiations are consistent with previous studies using DTI and TBSS in preterm neonates that showed a relationship between severe ROP and delayed white matter microstructural development in the optic radi-ations at term-equivalent age, independent of white matter injury.32 33 Further research at 7 years of age showed delayed optic radiation microstructure in children with a history of severe ROP compared with those with milder ROP.32 We have shown that these delays are present in the late preterm period and involve non-visual pathways, highlighting an early link of severe ROP with poor white matter maturation in preterm neonates.
Retinal nerve fibre layer (RNFL) thickness, assessed with optical coherence tomography, has been shown to be inversely associated with the stage of ROP, with the greatest involvement in severe ROP.34 In considering a relationship between white matter maturation and retinal development, previous research has shown that thinner RNFL thickness across the papillomac-ular bundle correlated with lower 18-month to 24-month CA cognitive and motor developmental scores.35 These findings provide insight into the associations between the retina and
the underlying white matter pathways, and offer a ‘window into the brain’ of the connections that the retinal ganglion and photoreceptor cells share with the white matter pathways. The maturational delays in the motor, visual and visual-association pathways of the developing brain detected in neonates with severe ROP suggest a mechanism by which these factors may act on neurodevelopment.
limitationsAlthough we were able to compare a large number of extremely preterm neonates with serial MRI scans, the timing of the follow-up MRI scans may have affected the imaging results due to the development of ROP over time as a progressively acquired disorder. We were unable to control for the timing of the ROP retinal laser therapy and its possible impact on the brain imaging findings. Visual acuity follow-up was not standardised across the cohort or done in conjunction with the 18-month CA neurode-velopmental assessments.
cOnclusIOnsSevere ROP requiring laser photocoagulation therapy is asso-ciated with delayed maturation in the motor, visual and visu-al-association pathways. Severe ROP predicted lower motor and cognitive functioning at 18 months’ CA, independent of severe brain injury and GA at birth. More research is needed to determine which potential mechanisms in severe ROP prevent optimal neurodevelopment and to assess the impacts of early and effective treatment of severe ROP on brain maturation.Author affiliations1Department of Pediatrics (Neurology), University of Toronto and the Hospital for Sick Children, Toronto, Canada2Neurosciences & Mental Health, SickKids Research Institute, Toronto, Canada3BC Children’s Hospital Research Institute, Vancouver, Canada4Department of Ophthalmology and Vision Science, University of British Columbia and BC Children’s Hospital, Vancouver, Canada5Department of Anesthesiology, University of Calgary, Calgary, Canada6Department of Pediatrics (Developmental Pediatrics), University of British Columbia and BC Children’s and Women’s Hospitals, Vancouver, Canada7Department of Occupational Science and Occupational Therapy, Vancouver, Canada8Sunny Hill Health Centre for Children, Vancouver, Canada9Department of Pediatrics (Neonatology), University of British Columbia and BC Children’s and Women’s Hospitals, Vancouver, Canada10Department of Radiology, University of British Columbia and BC Children’s Hospital, Vancouver, Canada
Acknowledgements We thank the children and their parents who generously committed their time and energy to participate in this study. Thank you to the clinical support staff in the paediatric ophthalmology clinic for their assistance in collecting the clinical ROP assessments. We would also like to thank the committed work of the therapists and physicians of the Neonatal Follow-up Program at the BC Women’s Hospital for their invaluable work assessing these children. We also would like to thank Janet Rigney, Sandra Belanger, RN, and Mark Chalmers, RRT, for their research support and work on this study.
contributors TJAG and VC had full access to all of the data in the study and take responsibility for the integrity of the data and the accuracy of the data analysis. Study design and conduct of the study: TJAG, VC, JG, SPM. Collection, management, analysis and interpretation of the data: TJAG, VC, JG, AS, JGZ, JV, REG, JF, KJP, SPM. Drafting of the manuscript: TJAG. Critical revision of the manuscript for important intellectual content: VC, JG, AS, JGZ, JV, REG, SPM. Statistical analysis: TJAG, VC, SPM. Administrative, technical or material support: TJAG, VC, JG, AS, JGZ, REG, SPM.
Funding Canadian Institutes for Health Research (CIHR) operating grant MOP-79262 (SPM) and MOP-86489 (REG). SPM is supported by the Bloorview Children’s Hospital Chair in Pediatric Neuroscience. REG holds a Senior Scientist Salary Award from the BC Children’s Hospital Research Institute. JGZ is funded by the Michael Smith Foundation, Canadian Child Health Clinician Scientist Program and CIHR. JV is supported by the Louise and Allan Edward Foundation. TJAG’s research funding is provided by the UBC Clinician Investigator Program and is currently an MSc student of the University of Toronto.
group.bmj.com on March 31, 2018 - Published by http://fn.bmj.com/Downloaded from

F537Glass TJA, et al. Arch Dis Child Fetal Neonatal Ed 2017;102:F532–F537. doi:10.1136/archdischild-2016-312533
Original article
competing interests None declared.
Patient consent Consent obtained from guardian.
ethics approval University of British Columbia/ Women’s and Children’s Research Ethics Board.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement Unpublished data from this study are not currently available to researchers outside of the study team approved by our research ethics committees.
© Article author(s) (or their employer(s) unless otherwise stated in the text of the article) 2017. All rights reserved. No commercial use is permitted unless otherwise expressly granted.
RefeRences 1 Lee J, Dammann O. Perinatal infection, inflammation, and retinopathy of prematurity.
Semin Fetal Neonatal Med 2012;17:26–9. 2 Gunther JB, Altaweel MM. Bevacizumab (Avastin) for the treatment of ocular disease.
Surv Ophthalmol 2009;54:372–400. 3 Schmidt B, Asztalos EV, Roberts RS, et al. Impact of bronchopulmonary dysplasia, brain
injury, and severe retinopathy on the outcome of extremely low-birth-weight infants at 18 months: results from the trial of indomethacin prophylaxis in preterms. JAMA 2003;289:1124–9.
4 Bassler D, Stoll BJ, Schmidt B, et al. Using a count of neonatal morbidities to predict poor outcome in extremely low birth weight infants: added role of neonatal infection. Pediatrics 2009;123:313–8.
5 Hellström A, Smith LE, Dammann O. Retinopathy of prematurity. Lancet 2013;382:1445–57.
6 Harrell SN, Brandon DH. Retinopathy of prematurity: the disease process, classifications, screening, treatment, and outcomes. Neonatal Netw 2007;26:371–8.
7 Schmidt B, Davis PG, Asztalos EV, et al. Association between severe retinopathy of prematurity and nonvisual disabilities at age 5 years. JAMA 2014;311:523–4.
8 Chau V, Synnes A, Grunau RE, et al. Abnormal brain maturation in preterm neonates associated with adverse developmental outcomes. Neurology 2013;81:2082–9.
9 Papile LA, Burstein J, Burstein R, et al. Incidence and evolution of subependymal and intraventricular hemorrhage: a study of infants with birth weights less than 1,500 gm. J Pediatr 1978;92:529–34.
10 Adams E, Chau V, Poskitt KJ, et al. Tractography-based quantitation of corticospinal tract development in premature newborns. J Pediatr 2010;156:882–8.
11 Chau V, Poskitt KJ, McFadden DE, et al. Effect of chorioamnionitis on brain development and injury in premature newborns. Ann Neurol 2009;66:155–64.
12 Duerden EG, Foong J, Chau V, et al. Tract-based spatial statistics in preterm-born neonates predicts cognitive and motor outcomes at 18 months. AJNR Am J Neuroradiol 2015;36:1565–71.
13 Brummelte S, Grunau RE, Chau V, et al. Procedural pain and brain development in premature newborns. Ann Neurol 2012;71:385–96.
14 International Committee for the Classification of Retinopathy of Prematurity. The international classification of retinopathy of prematurity revisited. Arch Ophthalmol 2005;123:991–9.
15 Early treatment of retinopathy of prematurity cooperative group. Revised indications for the treatment of retinopathy of prematurity. Arch Ophthalmol 2003;121:1684–96.
16 Chau V, Brant R, Poskitt KJ, et al. Postnatal infection is associated with widespread abnormalities of brain development in premature newborns. Pediatr Res 2012;71:274–9.
17 Bell M, Ternberg J, Feigin R, et al. Therapeutic decisions based upon clinical staging. Annals of Surgery 1978;187:1–7.
18 Miller SP, Ferriero DM, Leonard C, et al. Early brain injury in premature newborns detected with magnetic resonance imaging is associated with adverse early neurodevelopmental outcome. J Pediatr 2005;147:609–16.
19 Mukherjee P, Miller JH, Shimony JS, et al. Diffusion-tensor MR imaging of gray and white matter development during normal human brain maturation. AJNR Am J Neuroradiol 2002;23:1445–56.
20 Miller SP, Vigneron DB, Henry RG, et al. Serial quantitative diffusion tensor MRI of the premature brain: development in newborns with and without injury. J Magn Reson Imaging 2002;16:621–32.
21 Beaulieu C. The basis of anisotropic water diffusion in the nervous system - a technical review. NMR Biomed 2002;15:435–55.
22 Drobyshevsky A, Song SK, Gamkrelidze G, et al. Developmental changes in diffusion anisotropy coincide with immature oligodendrocyte progression and maturation of compound action potential. J Neurosci 2005;25:5988–97.
23 Smith SM, Jenkinson M, Johansen-Berg H, et al. Tract-based spatial statistics: voxelwise analysis of multi-subject diffusion data. Neuroimage 2006;31:1487–505.
24 Counsell SJ, Maalouf EF, Fletcher AM, et al. MR imaging assessment of myelination in the very preterm brain. AJNR Am J Neuroradiol 2002;23:872–81.
25 Bayley N. The bayley scales of infant development III. New York, New York: Psychological Corporation, 2005.
26 StataCorp. Stata statistical software. Release 14 2015. College Station, TX: StataCorp LP.
27 Cheng CM, Reinhardt RR, Lee WH, et al. Insulin-like growth factor 1 regulates developing brain glucose metabolism. Proc Natl Acad Sci U S A 2000;97:10236–41.
28 Joseph D’Ercole A, Ye P. Expanding the mind: insulin-like growth factor I and brain development. Endocrinology 2008;149:5958–62.
29 Hansen-Pupp I, Hövel H, Hellström A, et al. Postnatal decrease in circulating insulin-like growth factor-I and low brain volumes in very preterm infants. J Clin Endocrinol Metab 2011;96:1129–35.
30 Hansen-Pupp I, Holger H, Lofqvist C, et al. Circulatory IGF1 and brain volumes with neurodevelopment in preterm infants. Pediatr Res 2013;74:564–9.
31 Schmidt B, Roberts RS, Davis PG, et al; Caffeine for Apnea of Prematurity (CAP) Trial Investigators Caffeine for Apnea of Prematurity CAP Trial Investigators. Prediction of late death or disability at age 5 years using a count of 3 neonatal morbidities in very low birth weight infants. J Pediatr 2015;167:982–6.
32 Thompson DK, Thai D, Kelly CE, et al. Alterations in the optic radiations of very preterm children-perinatal predictors and relationships with visual outcomes. Neuroimage Clin 2014;4:145–53.
33 Bassi L, Ricci D, Volzone A, et al. Probabilistic diffusion tractography of the optic radiations and visual function in preterm infants at term equivalent age. Brain 2008;131:573–82.
34 Park KA, Oh SY. Retinal nerve fiber layer thickness in prematurity is correlated with stage of retinopathy of prematurity. Eye 2015;29:1594–602.
35 Rothman AL, Sevilla MB, Mangalesh S, et al. Thinner retinal nerve fiber layer in very preterm versus term infants and relationship to brain anatomy and neurodevelopment. Am J Ophthalmol 2015;160:1296–308.
group.bmj.com on March 31, 2018 - Published by http://fn.bmj.com/Downloaded from

neurodevelopmentdelayed white matter maturation and poorer Severe retinopathy of prematurity predicts
Steven P MillerJill G Zwicker, Ruth E Grunau, Anne Synnes, Kenneth J Poskitt and Torin J A Glass, Vann Chau, Jane Gardiner, Justin Foong, Jillian Vinall,
doi: 10.1136/archdischild-2016-312533published online May 23, 2017
2017 102: F532-F537 originallyArch Dis Child Fetal Neonatal Ed
http://fn.bmj.com/content/102/6/F532Updated information and services can be found at:
These include:
References http://fn.bmj.com/content/102/6/F532#ref-list-1
This article cites 33 articles, 6 of which you can access for free at:
serviceEmail alerting
box at the top right corner of the online article. Receive free email alerts when new articles cite this article. Sign up in the
Notes
http://group.bmj.com/group/rights-licensing/permissionsTo request permissions go to:
http://journals.bmj.com/cgi/reprintformTo order reprints go to:
http://group.bmj.com/subscribe/To subscribe to BMJ go to:
group.bmj.com on March 31, 2018 - Published by http://fn.bmj.com/Downloaded from