LA CITOGENÉTICA EN LOS LINFOMAS. UNA PERSPECTIVA …
58
LA CITOGENÉTICA EN LOS LINFOMAS. UNA PERSPECTIVA DESDE LA EXPERIENCIA Blanca Espinet Citogenètica Molecular, Servei de Patologia IMIM-Hospital del Mar
Transcript of LA CITOGENÉTICA EN LOS LINFOMAS. UNA PERSPECTIVA …
LA CITOGENÉTICA EN LOS LINFOMAS.
UNA PERSPECTIVA DESDE LA EXPERIENCIA
Blanca Espinet
Citogenètica Molecular, Servei de Patologia
IMIM-Hospital del Mar

CONSIDERACIONES TÉCNICAS
• Es esencial estudiar el tejido infiltrado por el
clon neoplásico
– Ganglio linfático: linfomas
– Sangre periférica: LLC y linfomas leucemizados
– Médula ósea: linfomas con infiltración medular
– Otros tejidos: bazo, estómago/intestino, líquidos
biológicos, en caso de infiltración
CONSIDERACIONES TÉCNICAS
• Citogenética convencional. Tipo de cultivo segun la
madurez de las células
– Células inmaduras:
• Cultivos directos (Burkitt)
• Cultivos de 24h sin mitógeno (LDCG)
– Células maduras:
• Cultivos de 72h+mitógeno (LLC, LF, LM, LEZM...)
• FISH en tejidos
– Selección correcta del tejido. Selección area problema
– Optimización de la técnica: pretratamientos y digestión
– Selección correcta de la sonda a aplicar

IMPORTANCIA DEL ESTUDIO GENÉTICO
DE LAS NEOPLASIAS LINFOIDES
• Diagnóstico. Clasificación OMS
• Pronóstico. Estratificación de pacientes
• Seguimiento de la enfermedad
• Tratamiento. Desarrollo de nuevos fármacos
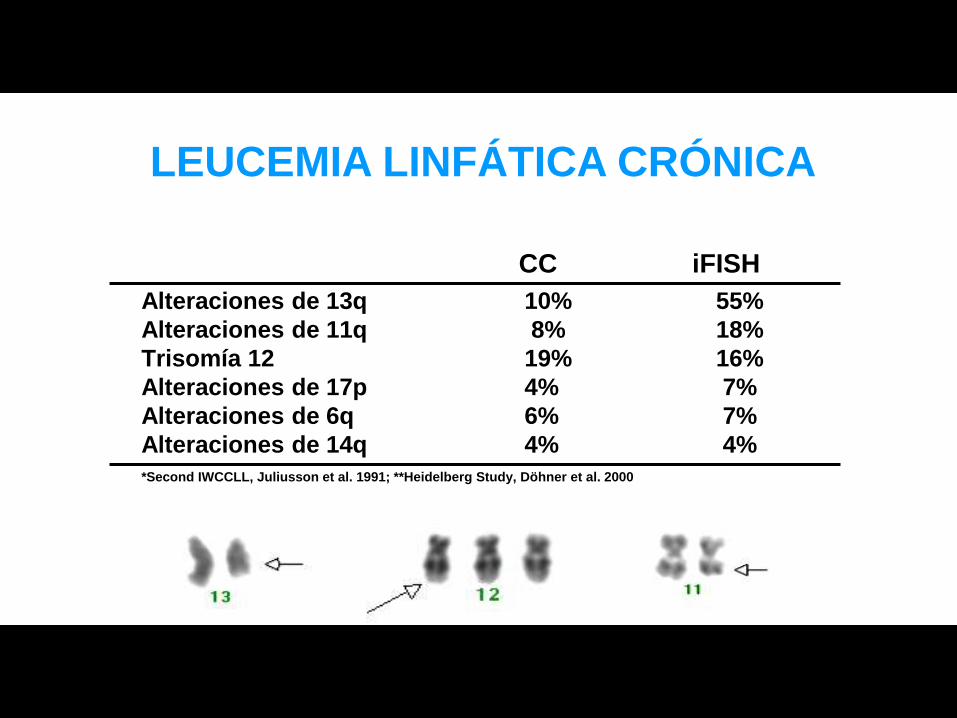
Alteraciones de 13q 10% 55%
Alteraciones de 11q 8% 18%
Trisomía 12 19% 16%
Alteraciones de 17p 4% 7%
Alteraciones de 6q 6% 7%
Alteraciones de 14q 4% 4%
*Second IWCCLL, Juliusson et al. 1991; **Heidelberg Study, Döhner et al. 2000
CC iFISH
LEUCEMIA LINFÁTICA CRÓNICA
LEUCEMIA LINFÁTICA CRÓNICA
• Alteraciones citogenéticas en la LLC
– Ninguna alteración es específica de esta patología:
NO BIOMARCADORES DIAGNÓSTICOS
– Porcentajes de casos alterados variables según la
técnica utilizada (CC ó FISH)
– Dificultad de obtener metafases del linfocito B tumoral
– Alteraciones pequeñas, crípticas por CC
FISH
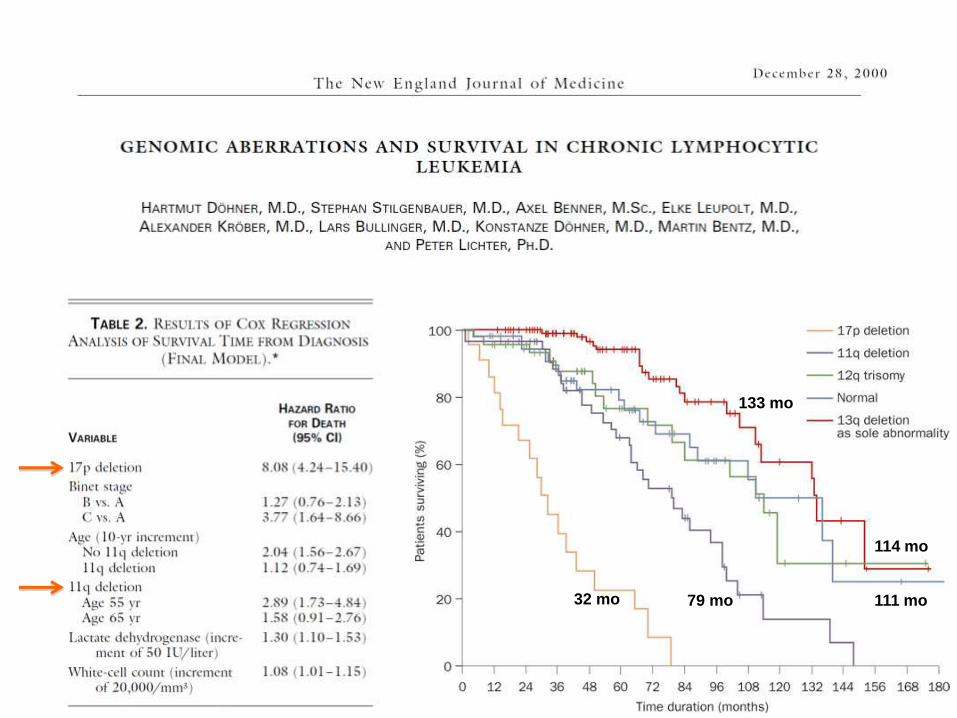
79 mo 32 mo
114 mo
111 mo
133 mo
| 364 | haematologica | 2009; 94(3)
Original Article
Acknowledgments: we thankall the physicians from theSpanish hospitals who con-tributed clinical data; we arealso grateful to Eva Lumbreras,María Pozo,Teresa Prieto,María Ángeles Hernández,AnaSimón,Ana Díez, and AlmudenaMartín, from “Centro deInvestigación del Cáncer,Salamanca” for their technicalassistance.
Funding: partially supportedby grants from “Proyectos deInvestigación Biomédica delSACYL” 106/A/06; "Ayudapredoctoral FIS de formaciónen investigación" (AR),FI06/00126 and by the"Acción Transversal del Cáncer"project, through an agreementbetween the Instituto de SaludCarlos III (ISCIII), the SpanishMinistry of Science andInnovation, and the CancerResearch Foundation ofSalamanca University”andRedes de Investigación RTIIC(FIS).
Manuscript received August 27,2008.Revised version arrivedOctober 17,2008.Manuscriptaccepted November 11,2008.
Correspondence: Jesús María Hernández,Servicio de Hematología yDepartamento de MedicinaHospital Universitario deSalamanca Paseo San Vicente58,37007 Salamanca, Spain.E-mail: [email protected]
Background
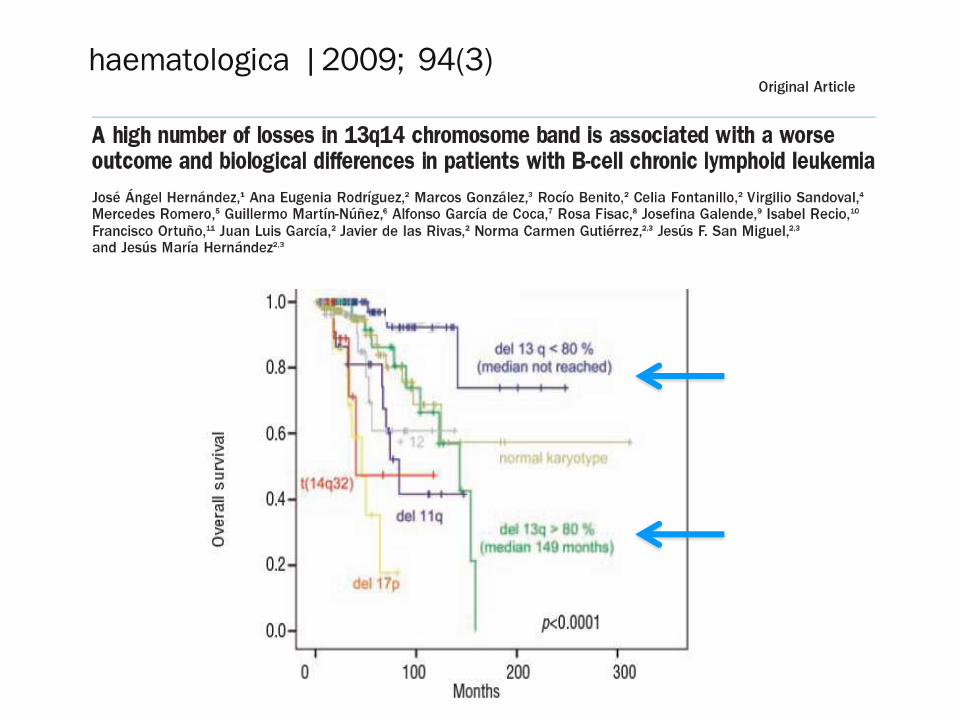
Among patients with B-cell chronic lymphoid leukemia, those with 13q14 deletion have
a favorable outcome. However, whether the percentage of cells with 13q- influences the
prognosis or the biological characteristics of this disease is unknown. We analyzed the
clinico-biological characteristics and outcome of patients with B-cell chronic lymphoid
leukemia with loss of 13q as the sole cytogenetic aberration.
Design and Methods
Three hundred and fifty patients with B-cell chronic lymphoid leukemia were studied.
Clinical data were collected and fluorescence in situ hybridization and molecular studies
were carried out. In addition, a gene expression profile was obtained by microarray-based
analysis.
Results
In 109 out of the 350 cases (31.1%) loss of 13q was the sole cytogenetic aberration at diag-
nosis. In the subgroup of patients with 80% or more of cells with loss of 13q (18 cases),
the overall survival was 56 months compared with not reached in the 91 cases in whom
less than 80% of cells had loss of 13q (p< 0.0001). The variables included in the multivari-
ate analysis for overall survival were the percentage of losses of 13q14 (p=0.001) and B
symptoms (p=0.007). The time to first therapy in the group with 80% or more vs. less than
80% of losses was 38 months vs. 87 months, respectively (p=0.05). In the multivariate
analysis the variables selected were unmutated status of IgVH (p=0.001) and a high level of
b2microglobulin (p=0.003). Interestingly, these differences regarding overall survival and
time to first therapy were also present when other cut-offs were considered. The gene
expression profile of patients with a high number of losses in 13q14 showed a high pro-
liferation rate, downregulation of apoptosis-related genes, and dysregulation of genes
related to mitochondrial functions.
Conclusions
Patients with B-cell chronic lymphoid leukemia with a high number of losses in 13q14 as
the sole cytogenetic aberration at diagnosis display different clinical and biological features:
short overall survival and time to first therapy as well as more proliferation and less apop-
tosis. A quantification of the number of cells showing a genetic abnormality should, there-
fore, be included in the study of the prognostic factors of B-cell chronic lymphoid leukemia.
Key words: B chronic lymphoid leukemia, 13q14 deletion, outcome, proliferation, apop-
tosis.
Citation: Hernández JA, Rodríguez AE, González M, Benito R, Fontanillo C, Sandoval V, RomeroM, Martín-Núñez G, de Coca AG, Fisac R, Galende J, Recio I, Ortuño F, García JL, de las RivasJ, Gutiérrez NC, San Miguel JF, and Hernández JM. A high number of losses in 13q14 chromo-some band is associated with a worse outcome and biological differences in patients with B chroniclymphoid leukemia.Haematologica 2009; 94:364-371. doi:10.3324/haematol.13862
©2009 Ferrata Storti Foundation. This is an open-access paper.
A high number of losses in 13q14 chromosome band is associated with a worseoutcome and biological differences in patients with B-cell chronic lymphoid leukemia
José Ángel Hernández,1 Ana Eugenia Rodríguez,2 Marcos González,3 Rocío Benito,2 Celia Fontanillo,2 Virgilio Sandoval,4
Mercedes Romero,5 Guillermo Martín-Núñez,6 Alfonso García de Coca,7 Rosa Fisac,8 Josefina Galende,9 Isabel Recio,10
Francisco Ortuño,11 Juan Luis García,2 Javier de las Rivas,2 Norma Carmen Gutiérrez,2,3 Jesús F. San Miguel,2,3
and Jesús María Hernández2,3
1Servicios de Hematología, Hospital Infanta Leonor, Madrid; 2IBMCC, Centro de Investigación del Cáncer, Universidad de Salamanca-CSIC; 3Hospital Clínico Universitario de Salamanca; 4Hospital Virgen Blanca, León; 5Hospital del Río Hortega, Valladolid;6Hospital Virgen del Puerto, Plasencia, Cáceres; 7Hospital Clínico Universitario, Valladolid; 8Hospital General de Segovia; 9Hospital del Bierzo, León; 10Hospital Nuestra Señora de Sonsoles, Ávila, and 11Hospital Morales Meseguer, Murcia, Instituto de Estudios deCiencias de la Salud de Castilla y León (IECSCYL), Unidad de Investigación, Hospital Universitario de Salamanca, Spain
ABSTRACT

¿RESURGIMIENTO
DE LA CITOGENÉTICA CONVENCIONAL
EN LA LLC?
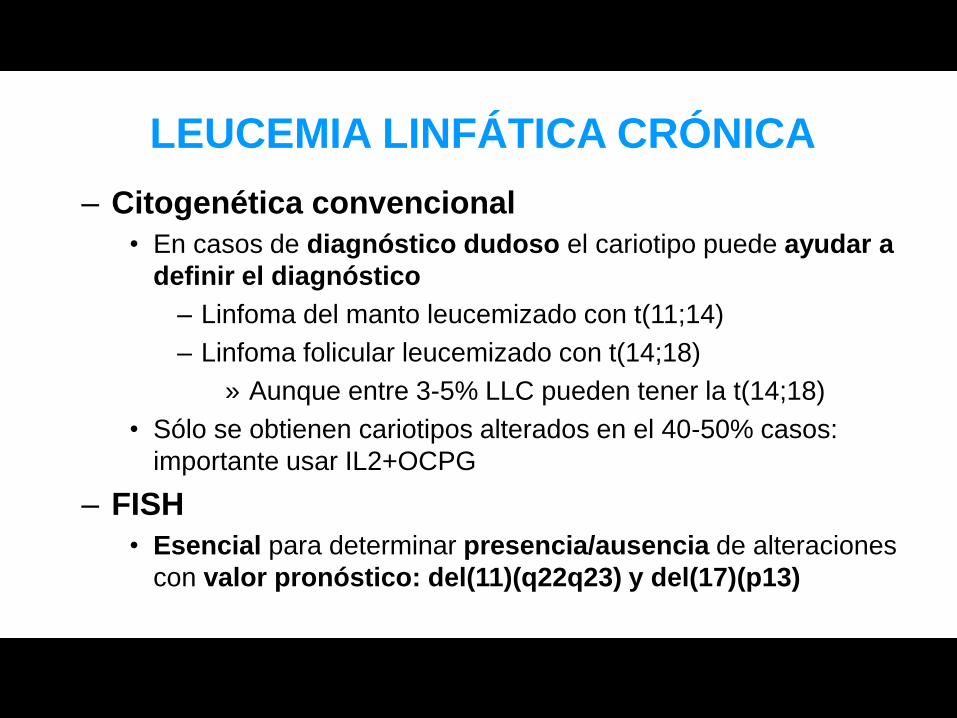
– Citogenética convencional
• En casos de diagnóstico dudoso el cariotipo puede ayudar a
definir el diagnóstico
– Linfoma del manto leucemizado con t(11;14)
– Linfoma folicular leucemizado con t(14;18)
» Aunque entre 3-5% LLC pueden tener la t(14;18)
• Sólo se obtienen cariotipos alterados en el 40-50% casos:
importante usar IL2+OCPG
– FISH
• Esencial para determinar presencia/ausencia de alteraciones
con valor pronóstico: del(11)(q22q23) y del(17)(p13)
LEUCEMIA LINFÁTICA CRÓNICA

TRANSLOCACIONES CROMOSÓMICAS
DE LOS LINFOMAS B
Las translocaciones en los linfomas B
afectan mayoritariamente a los genes de las
inmunoglobulinas:
cadena pesada, IGH
cadenas ligeras, IGK e IGL

t(14;18)(q32;q21)
t(2;18)(p11;q21)
t(18;22)(q21;q11)
•LF (85%)
•LDCG (12-30%)
•Linfomas “doble hit” (15%)
BCL2
CCND1 •LCM (90-95%%) t(11;14)(q13;q32)
MYC
•LB (90-100%)
•LDCG (10%)
•Linfomas doble hit (35-50%)
t(8;14)(q24;q32)
t(2;8)(p11;q24)
t(8;22)(q24;q11)
BCL6
•LDCG (30-40%)
•LF (15%)
•Linfomas doble/triple hit (5-10%)
t(3;v)(q27;v)
t(11;18)(q21;q21)
t(14;18)(q32;q21) MALT1 •L MALT (20-50%)

LINFOMA FOLICULAR
– Alteración primaria: t(14;18)(q32;q21), IGH/BCL2 • Incidencia variable según grado histológico
– 85-90% LF grados 1 y 2
– 75% LF grado 3A
– 15% LF grado 3B
– Variantes t(2;18)(p11;q21) y t(18;22)(q21;q11) poco frecuentes
• t(14;18) muy característica pero no específica del LF
– 15-30% LDCG
– 5% LLC
– t(14;18) IGH/MALT1 cromosómicamente idéntica
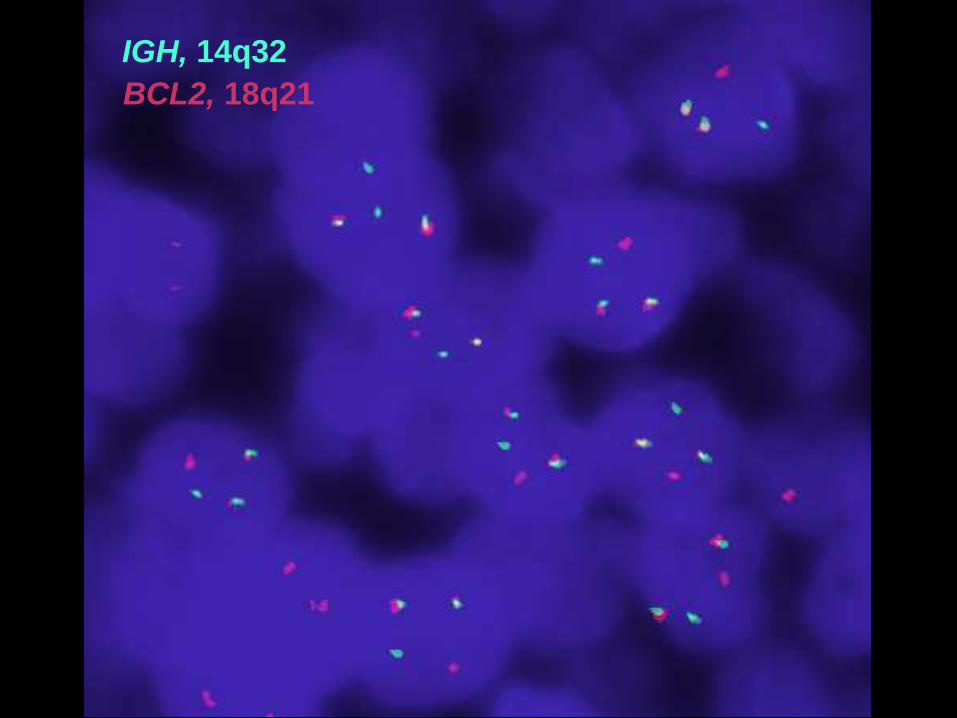
IGH, 14q32
BCL2, 18q21

46,XY,der(4),del(7)(q22),del(10)(q22),inv(11)(p11q25)

IGH, 14q32
BCL2, 18q21
LINFOMA FOLICULAR
– Alteraciones secundarias, 90% casos
• +7, +8, +12, +3, +18, +X, 10-20% casos
• t(3;V)(q27;V), BCL6, 5-15%, grados 3B
• del(6)(q21), 60% FISH
• del(17)(p13), 20% FISH
• Cariotipos complejos: pronóstico desfavorable


– Alteración primaria: t(11;14)(q13;q32), IGH/CCND1
• Alteración altamente específica de LCM
• Incidencia
– 65-70% CC
– 90-95% FISH
– 40-70% PCR, según primers utilizados
• Se ha descrito también en Mieloma Múltiple
• Raramente t(2;11)(p11;q13) ó t(11;22)(q12;q11)
• 5% de LCM no presentan la t(11;14)(q13;q32): CCND1-
LINFOMA DE CÉLULAS DEL MANTO
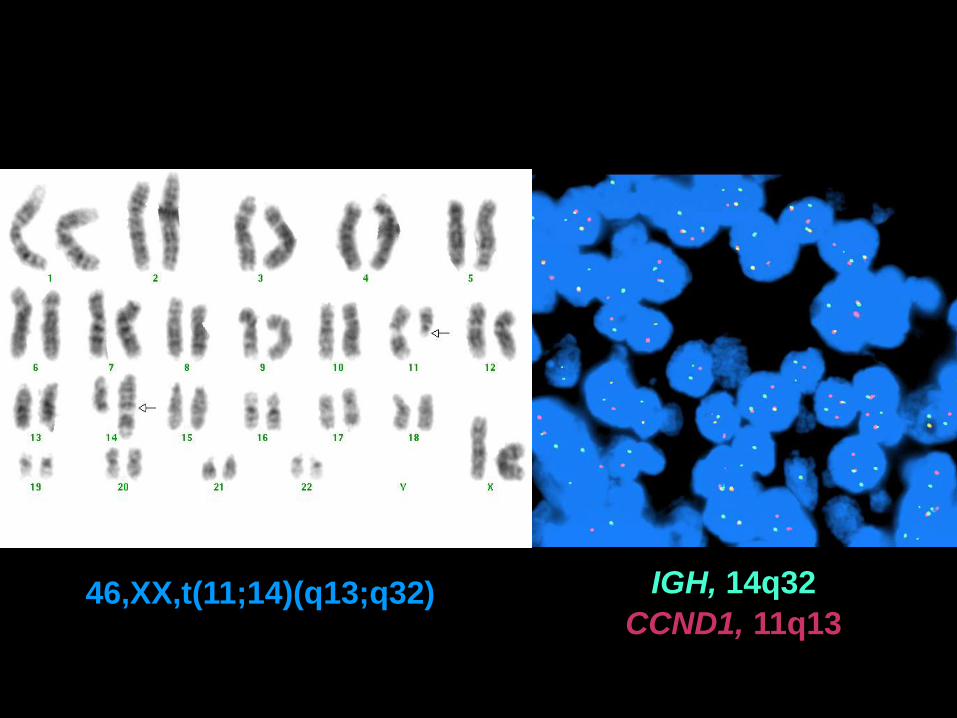
IGH, 14q32
CCND1, 11q13 46,XX,t(11;14)(q13;q32)

55%
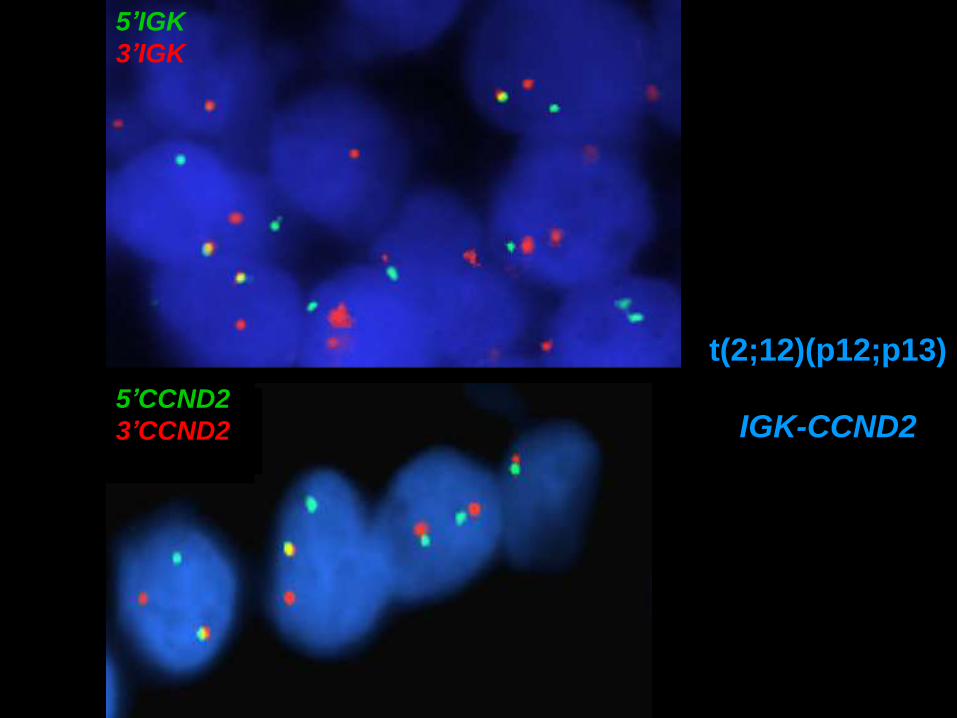
5’IGK
3’IGK
5’CCND2
3’CCND2
t(2;12)(p12;p13)
IGK-CCND2

Alteraciones secundarias, 50-90%

PRONÓSTICO DE LAS ALTERACIONES SECUNDARIAS,
CITOGENÉTICA CONVENCIONAL
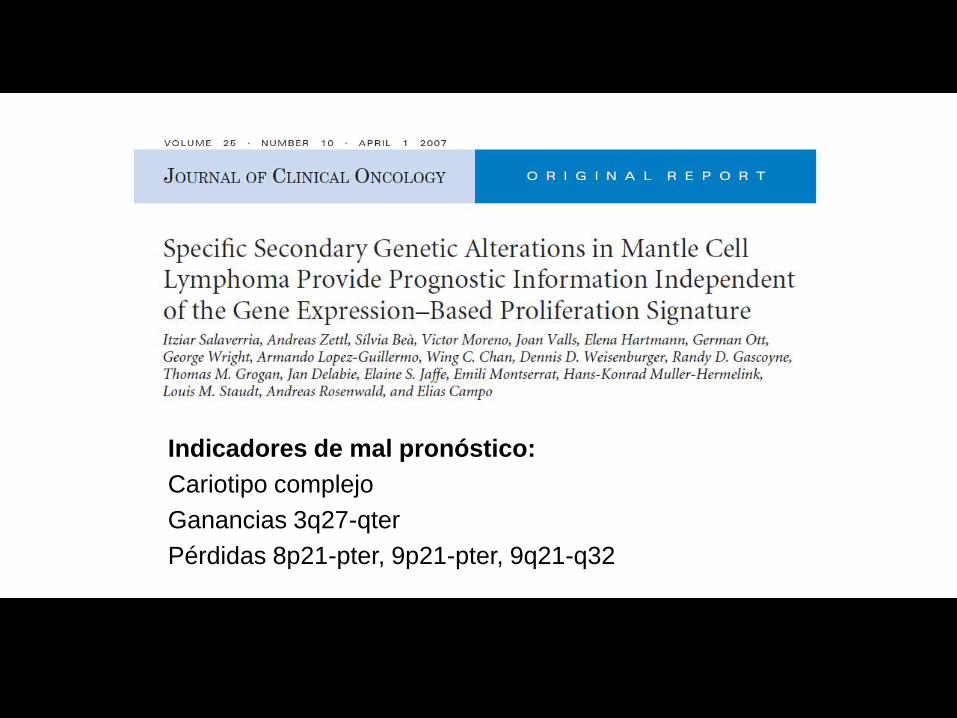
Indicadores de mal pronóstico:
Cariotipo complejo
Ganancias 3q27-qter
Pérdidas 8p21-pter, 9p21-pter, 9q21-q32
LINFOMA DE LA ZONA MARGINAL
EXTRANODAL TIPO MALT
• Alteraciones citogenéticas más frecuentes
– t(11;18)(q21;q21), API2/MALT
• Incidencia 20-50%
• Linfoma MALT gástrico y pulmonar
• Resistencia a terapia erradicadora de Helicobacter
pylori: Biomarcador predictivo de respuesta
– t(14;18)(q32;q21), IGH/MALT
• Incidencia 10-20%
• Linfoma MALT de conjuntiva/órbita y glándula
salival, piel (?)
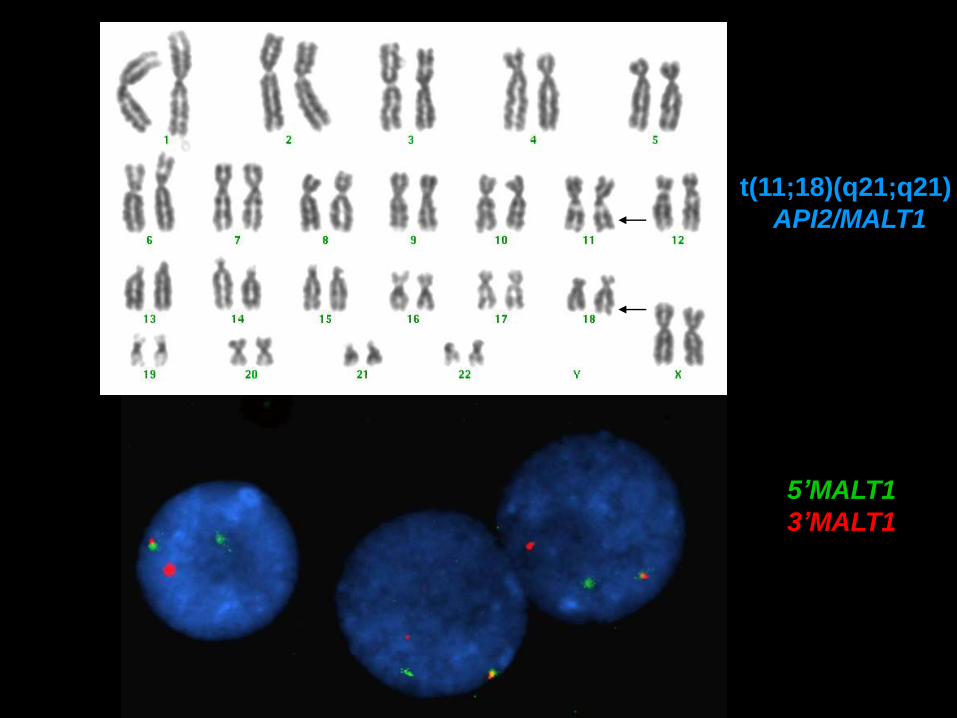
t(11;18)(q21;q21)
API2/MALT1
5’MALT1
3’MALT1
LINFOMA DE LA ZONA MARGINAL
EXTRANODAL TIPO MALT
• Otras alteraciones citogenéticas
– t(1;14)(p22;q32), IGH/BCL10
• Incidencia 5%
• Linfomas MALT de alto grado
– t(3;14)(p14;q32), IGH/FOXP1
• Incidencia 10%
• Linfoma MALT de conjuntiva/órbita, tiroides, piel (?)
• Nunca en estómago, glándula salival y en otros
linfomas marginales
– Trisomías 3 y 18
• +3: 20-60%,variable según tipo de tejido y series.
No papel en progresión
• +18: más frecuente en linfomas MALT de alto grado
– Alteraciones primarias • t(14;18)(q32;q21), IGH/BCL2
– Incidencia 15-30%
– Casos que derivan de un LF previo
– La gran mayoría de casos presentan alteraciones secundarias asociadas
• t(3;V)(q27;V), BCL6
– Incidencia 5-10% CC; 20-30% FISH
– Gran variedad de parejas de reordenamiento: 14q32, 2p11, 22q11, 4p11, 6q21, 11q23
• t(8;14)(q24;q32), IGH/MYC
– Incidencia 7-10% CC+FISH
LINFOMA DIFUSO DE CÉLULA GRANDE
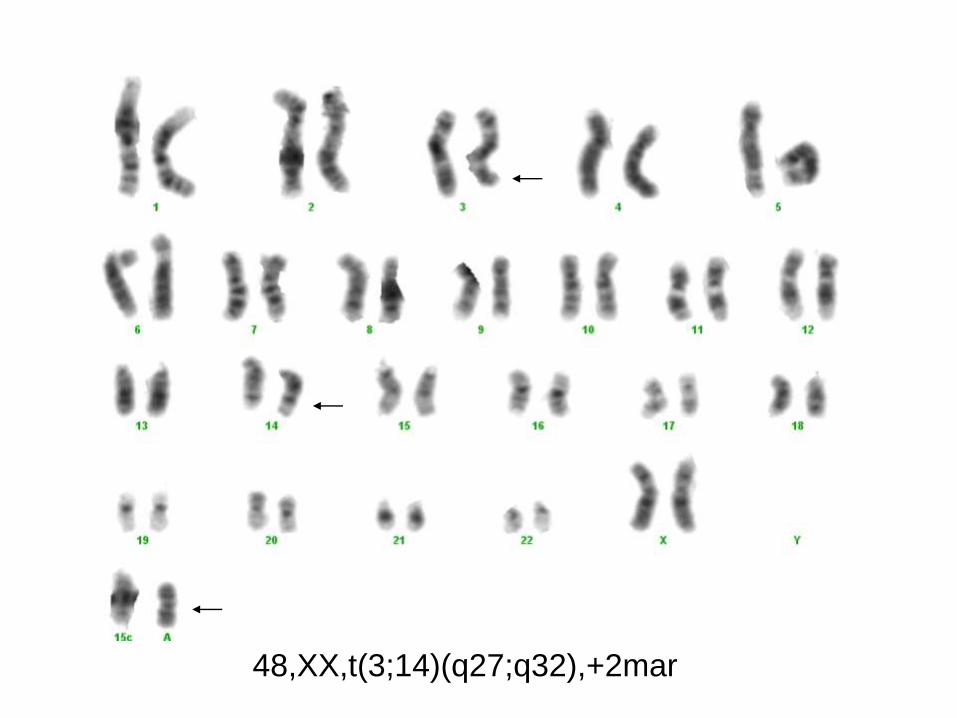
48,XX,t(3;14)(q27;q32),+2mar
– Alteraciones secundarias • Trisomías 3, 5, 6, 11, 12, 18 y X
• Ganancias 1q, 6p
• Deleciones 1p, 6q, 7q32-ter, 8p, 9p, 11q, 17p
• ABC: Ganancias 3/3q, 18q21-22, deleciones 6q21
• GCB: Ganancias 12p12
LINFOMA DIFUSO DE CÉLULA GRANDE
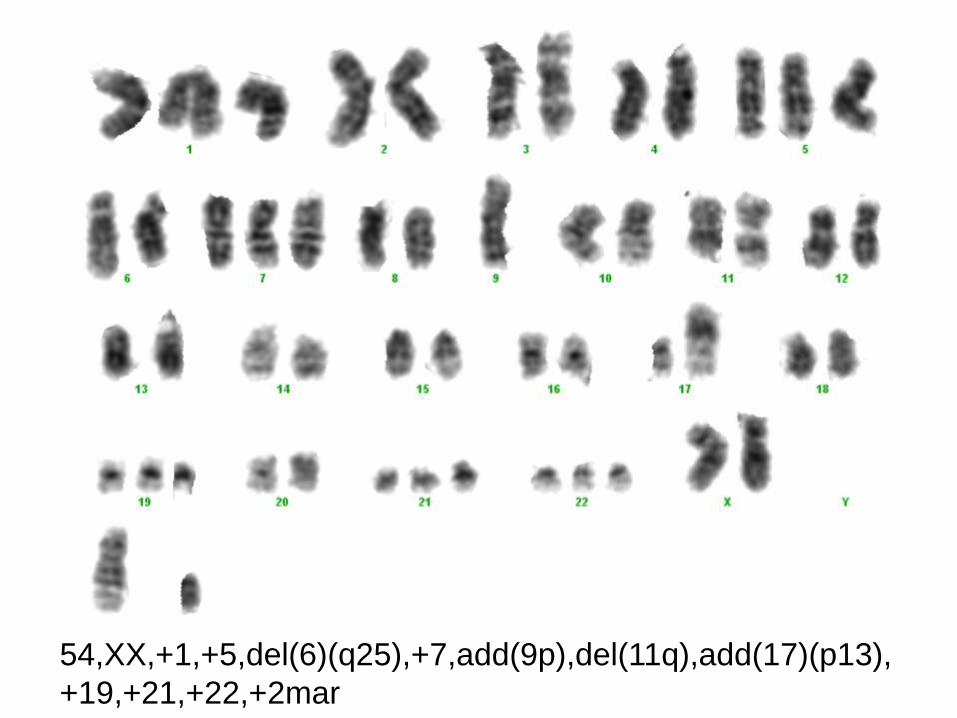
54,XX,+1,+5,del(6)(q25),+7,add(9p),del(11q),add(17)(p13),
+19,+21,+22,+2mar
• Valor pronóstico de las alteraciones citogenéticas
– Translocaciones de MYC: pronóstico desfavorable
– Dobles y triples “hits” (MYC, BCL2, BCL6): pronóstico
desfavorable cuando MYC implicado
– Translocaciones de BCL6 y BCL2: no valor pronóstico
LINFOMA DIFUSO DE CÉLULA GRANDE

LINFOMA DE BURKITT
– Alteracion primaria: t(8;14)(q24;q32), IGH/MYC • Característica pero no específica de LB: también en LDCG
• Incidencia 70-80%
• Variantes:
– t(2;8)(p11;q24),10-15%
– t(8;22)(q24;q11), 2-5%
• ≈10%: ausencia de translocación de MYC
• Punto de rotura de IGH/MYC muy variable, no PCR
– Formas endémicas: rotura en IGHV
– Formas esporádicas: rotura en IG switch region
LINFOMA DE BURKITT
– Alteraciones secundarias • Duplicaciones 1q21q25
• Deleciones 6q11q14
• Deleciones 17p13
• +12, +7, +8, +18
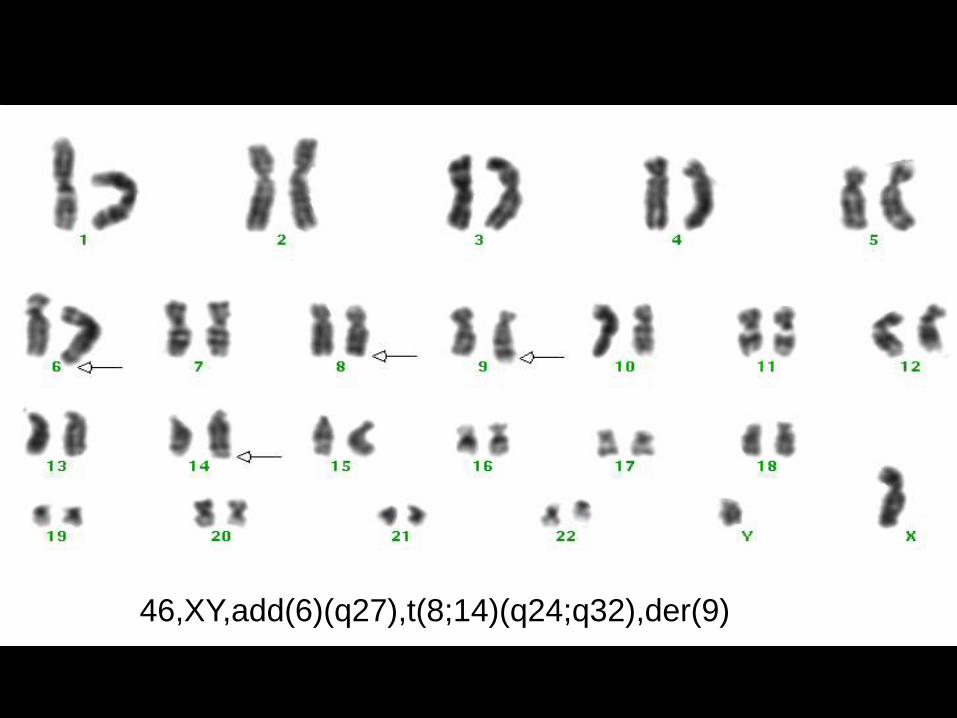
46,XY,add(6)(q27),t(8;14)(q24;q32),der(9)
• Citogenética convencional
– Importante seleccionar muestra tumoral y tipo cultivo
– Cultivo de ganglios limitado por cantidad de tejido
– Si obtenemos metafases pueden ser muy informativas
• FISH
– Elección de sonda según diagnóstico.
• Altamente específica
– Complementar con PCR.
• Muy sensible
• Seguimiento EMR
¿QUÉ ESTUDIOS CITOGENÉTICOS HACEMOS
EN LOS LINFOMAS?
CONSIDERACIONES TÉCNICAS
Para interpretar los resultados
citogenéticos siempre tener en cuenta: los
datos clínicos, citológicos, histológicos,
inmunofenotípicos y de biología molecular
DIAGNÓSTICO INTEGRADO

Laboratori de Citogenètica Molecular
Laboratori de Citologia Hematològica
Laboratori de Biologia Molecular
Servei de Patologia
Servei d’Hematologia Clínica
AGRADECIMIENTOS

Los biomarcadores pueden ser: proteínas (ej determinados antígenos),
perfiles genéticos, epigenéticos y de proteómica; proporcionan
información específica sobre un proceso de la enfermedad
• Marcador diagnóstico se basa en el reconocimiento inicial de
cáncer o bien en su recidiva.
• Marcador pronóstico proporciona información
perteneciente a la historia natural de la enfermedad, la
probabilidad de recidiva de la enfermedad y la duración de
la remisión. Independiente del tto.
• Marcador predictivo identifica la probabilidad de respuesta a un
agente o modalidad terapéutica específicos.
BIOMARCADORES

• Qué papel van a tener los arrays genómicos?
FISH: del(13q) y +12
CC: 49,XX,+12,+18,+19
Ventajas:
-Elevada resolución, detecta alt. pequeñas
-Informa de todo el genoma
Limitaciones:
-Sensibilidad baja: mín. 30% infiltración
-Precio? 150-500 euros
Array: del(13q), +12, +18, +19
LEUCEMIA LINFÁTICA CRÓNICA

• Detección Enfermedad Mínima Residual (EMR)
– El seguimiento de la EMR con técnicas de PCR cuantitativa a tiempo real
proporciona información sobre la cinética de aparición/desaparición de células
patológicas circulantes
• Los datos obtenidos pueden ser predictivos de recaída o remisión continuada
– La obtención de respuesta molecular (RM)
• disminuye el riesgo de recaída
• aumenta el tiempo libre de enfermedad
– La consecución de RM no es sinónimo de curación
– Con el estado de conocimiento actual, ¿la obtención de RM debe ser uno de los
objetivos del tratamiento?
– En el LF, el beneficio de conseguir RM está aún por dilucidar
• La t(14;18) se ha hallado en un 50% de indivíduos sanos, en proporciones
muy bajas, 10-4-10-6 !!
LINFOMA FOLICULAR
• Del(11q)
Poco detectada por CC (3%) vs FISH (18%)
Genes candidatos: ATM, RDX, PPP2R1B, IL1BC, Caspasas 1, 4 y 5
Correlaciones clínicas:
– individuos jóvenes, predominancia de sexo masculino
– estadios avanzados, adenomegalias
– resistencia al tratamiento
– rápida progresión de la enfermedad y supervivencia corta
LEUCEMIA LINFÁTICA CRÓNICA
LEUCEMIA LINFÁTICA CRÓNICA
• Del(17)(p13)
Poco frecuente de novo (2-4%), más frecuente en pacientes refractarios
a tratamiento (30%)
Genes implicados: TP53
Correlaciones clínicas
– Estadios avanzados, linfadenopatias, síntomas B
– Requerimiento rápido de tratamiento
– Resistencia al tratamiento, supervivencia corta

¿RESURGIMIENTO DE LA CITOGENÉTICA?

• LLC
– +12, del (13q), del (11q), del(17p): Ninguna exclusiva
– Pronóstico desfavorable: del(17)(p13), del(11)(q22q23)
• LZME
– del(7q), +3: no exclusivas
– No alteraciones claramente asociadas a pronóstico
• LMALT
– t(11;18): gástricos y pulmonares; resistencia tratamiento H. Pylori
– Otras poco frecuentes: t(14;18) IGH/MALT, t(1;14) IGH/BCL10, t(3;14) FOXP1/IGH
– Trisomías 3, 18
• LF
– t(14;18)(q32;q21), IGH/BCL2: característica pero no exclusiva
– 90% casos alteraciones secundarias
– No alteraciones claramente asociadas a pronóstico
• LM
– t(11;14)(q13;q32), CCND1/IGH: muy característica!
– Pronóstico desfavorable: +3q, del(17)(p13)
• LDCG
– t(14;18)(q32;q21), IGH/BCL2; t(3;V)(q27;V), BCL6; t(8;14)(q24;q32), IGH/MYC
– Cariotipos complejos
– Doble y triple hits: pronóstico desfavorable
• LB
– t(8;14)(q24;q32), IGH/MYC: característica pero no exclusiva
– 10% casos sin translocación MYC
¿Qué debemos recordar?