INVESTIGACION EN NUTRICION Y ALIMENTACIÓN … · SUMARIO DE ESTE NÚMERO Numeral ... centres would...
29
INVESTIGACION EN NUTRICION Y ALIMENTACIÓN PEDIÁTRICAS (Revista on-line) INVEST NUTR ALIM PEDIATR (Rev on-line) 2004; 2. #1-32. http:// www.seinap.org CONSEJO DE REDACCIÓN EDITORES - Director: M. Bueno M. Moya - Secretaria: M. Juste E. Cortés - Consejeros: A. Carrascosa, A. Gil, D. Infante, R. Leis y L. Ros ISSN: 1988-5997 SUMARIO DE ESTE NÚMERO Numeral Editorial: - M. Moya. The role of subspecialities in Pediatrics. #1 Artículos: - R. Tormo. Futuro de la nutrición enteral. #2 Abstracts SEINAP 04 #3-32 EDITORIAL - Moya, M. THE ROLE OF SUBSPECIALITIES IN PEDIATRICS. INVEST NUTR ALIM PEDIATR (Rev on- line) 2004; 2. #01. http:// www.seinap.org Recent interest in the Pediatric training in Spain has been manifested from two distant points in the world. Even in areas where child care comes under general pediatricians the tendency for Pediatric. Subspecialities is growing and becoming established with quite a few different methods. This is the reason for this account being published in the web. The concept of speciality and specialist in medicine encompasses clinical care including the study and/or treatment of a group of particular diseases. The trunk specialities are over a
Transcript of INVESTIGACION EN NUTRICION Y ALIMENTACIÓN … · SUMARIO DE ESTE NÚMERO Numeral ... centres would...

INVESTIGACION EN NUTRICION Y ALIMENTACIÓN PEDIÁTRICAS (Revista on-line)
INVEST NUTR ALIM PEDIATR (Rev on-line) 2004; 2. #1-32. http:// www.seinap.org
CONSEJO DE REDACCIÓN EDITORES
- Director: M. Bueno M. Moya
- Secretaria: M. Juste E. Cortés
- Consejeros: A. Carrascosa, A. Gil, D. Infante, R. Leis y L. Ros
ISSN: 1988-5997
SUMARIO DE ESTE NÚMERO Numeral
Editorial:- M. Moya. The role of subspecialities in Pediatrics.
#1
Artículos:- R. Tormo. Futuro de la nutrición enteral.
#2
Abstracts SEINAP 04 #3-32
EDITORIAL
- Moya, M.
THE ROLE OF SUBSPECIALITIES IN PEDIATRICS. INVEST NUTR ALIM PEDIATR (Rev on-line) 2004; 2. #01. http:// www.seinap.org
Recent interest in the Pediatric training in Spain has been manifested from two distant points in the world. Even in areas where child care comes under general pediatricians the tendency for Pediatric. Subspecialities is growing and becoming established with quite a few different methods. This is the reason for this account being published in the web.
The concept of speciality and specialist in medicine encompasses clinical care including the study and/or treatment of a group of particular diseases. The trunk specialities are over a

century old and the subspecialities have arisen more recently as consequence of increased knowledge but especially coming from more specific medical care. The branching that happened in Internal Medicine is an earlier phenomena and with its own peculiarities but has been a model for what has been happening in the last few decades in pediatrics. In the Occidental countries at present in Pediatrics the following organ or system subspecialities exist: Neonatology, Cardiology, Gastroenterology, Neurology, Endocrinology, Nephrology, Onco-hematology, Allergy, Infectology, Psychiatry, Genetics… among other non-organ ones but no less important. The development and denomination of these varies from country to country and is also subject to change. Some type of attendance grouped by age is beginning to disappear as is the case of the pre-school children or even infant wards in favour of the subspecialities mentioned.
In relation to pediatric subspecialities there is no regulating homogeneity as in undergraduate studies. In Europe two levels exist: One for each country which has its own rules and legislation, in Spain this is the National Board of Medical Specialities (Comisión Nacional de Especialidades Médicas) with its National Sub-Board of Pediatrics and its Sub-specialities (Comisión Nacional de Pediatría).
The second level would cover the whole European Community although it is more theoretical with general guidelines that are normally consulted. This level is not an official body of the European Union but made up by scientific organisations such as The Union of European Medical Specialists (UEMS) and European Specialists in Pediatrics (CESP). They have thoroughly thought up some ideal and very rigorous training programmes for sub-specialists that are difficult to adapt to the system of the country members Ministries of Health.
Training in Pediatric sub-specialities
As when dimensioning a new hospital service the main thing is a previous study of the expected number of incoming patients, here it is compulsory to approach the number of different sub-specialists for the next ten years. This is difficult to estimate and easily biased by project designers especially if they come from tertiary hospitals. Probably a global assessment of the country with varied population densities and hospital network could be a more rational way.
Neonatology training model
In 1994 the European Society for Pediatric Research drafted the European Training Syllabus in Neonatology. After a careful and elaborate process the last document (circa 1998) was accepted by CESP as fundamental for the training of neonatologists. However, the duration of three additional years following the regular three year period of residency; the identification or selection of tertiary care units and teachers; or the financial cost of these three years have made this programme come under careful scrutiny from different governments of the European Union. This is a unique example because there are no

synonymous sub-specialities in adult care. When dealing with other pediatric sub-specialities close cooperation with the adult counterpart should be considered. In Spain the traditional model has proved to be quite useful up to this moment but it needs modifying in terms of formation quality and the required number of specialists.
The sub-specialisation in Pediatrics is undoubtedly improving the diagnosis procedure and care of the sick child. Two questions arise in relation to sub-specialisation. First, how to carry out the training procedure and second, how to convince ourselves that only a minority from the 250 pediatricians yearly qualified in Spain (40 million) will practise as a real specialist. In the context it seems reasonable to approach models which are shorter and not so ambitious so becoming more affordable for both pediatricians and health administration. To shorten the pre-graduate medical studies and to lengthen the pediatric residency up to five years could be a reasonable issue. Perhaps we could contemplate providing a scheme with a prolonged stay in one of the clinical units caring for patients of one of the 12 mentioned subspecialties. Flexibility for rotation in other centres would complete this range.
The task which remains ahead of us is not an easy one. The content definition of neighbouring subspecialties or the highly specialised (invasive) techniques are a clear example.
To end we should go back to figures. In western countries in the last few decades there has been an increase in training and subsequent qualifications for general practitioners. In Spain in the next few years the ratio paediatrician/General Practitioner will be 1/20. In this context it is not madness to think that Child Primary Care could be removed from the pediatrician´s usual activities. The paediatrician would then become a consultant and would probably branch out into a very high quality training with rotation in specific fields, then this more selective role would be consolidated.
Reference: Moya M. An Pediatr 2003; 58 (Supl 4): 399-400
ARTICULOS.
R. TORMO. FUTURO DE LA NUTRICIÓN ENTERAL.INVEST NUTR ALIM PEDIATR (Rev on-line) 2004; 2. #02. http:// www.seinap.org

El progreso en el conocimiento de la fisiología digestiva, aporte, digestión y absorción de principios inmediatos, necesidades en situaciones especiales, tras procesos degenerativos del organismo, o tras intervenciones, o la mejor comprensión de situaciones fisiológicas como las que rodean al recién nacido, prematuro, embarazada, ancianidad, ha propiciado el desarrollo de técnicas de alimentación especiales que han contribuido a mejorar el estado nutritivo, evolución de ciertas enfermedades o el bienestar del paciente.
En un principio, esta pequeña revolución de la medicina se inició con la alimentación parenteral, para posteriormente desarrollarse la alimentación enteral, beneficiándose de investigaciones iniciadas en la alimentación en los viajes espaciales.
Las ventajas de esta última que pueden resumirse en que sobre todo no dejan de ejercer un efecto trófico sobre el intestino y se acoplan a las necesidades especiales de cada situación, se pueden conseguir, modificando tan solo la proporción de proteínas, grasas, carbohidratos y sales minerales, o bien con la adición de otros nutrientes o compuestos orgánicos o inorgánicos.
La divulgación de estos conocimientos y técnicas ha propiciado en nuestro país un interés sin duda beneficioso para el enfermo y la nutrición como ente, y una consecuencia sociológica, plasmada en lo que podríamos decir, “taifismo” , un sinnúmero de sociedades “taifas” de nutrición que me permito enumerar:
- Asociación Española de Diplomados en Enfermería de Nutrición y Dietética (ADENYD), As. Esp. De Dietistas y Nutricionistas (AEDN), As. Esp. De Doctores y Licenciados en Ciencia y Tecnología de los Alimentos (ALCYTA), Sociedad Española de Dietética y Ciencias de la Alimentación (SEDCA), Soc. Española de Endocrinología y Nutrición (SEEN), Soc. Española de Gastroenterología, Hepatología y Nutrición Pediátrica (SEGHNP), Sociedad Española de Nutrición (SEN), Sociedad Española de Nutrición Básica y Aplicada (SENBA), Sociedad Española de Nutrición Comunitaria (SENC), Soc. Española de Nutrición Enteral y Parenteral (SENP), Soc. Española de Investigación, Nutrición y Alimentación en Pediatría (SEINAP). Amén de los comités de Nutrición de cada una de las Sociedades regionales de Medicina o Pediatría.
Muchas de estas sociedades taifas están o quieren estar englobadas en un a modo de califato o sociedad tutelar llamado FESNAD (Federación Española de Sociedades de Nutrición, Alimentación y Dietética), esta vez no radicado en Córdoba sino centralizado en Madrid.
Sería interesante desde un punto de vista histórico, saber si esta tendencia al taifismo procede de la rama visigótica o musulmana de nuestra psique.
Cada una de estas sociedades consta, como es lógico, de presidente, secretario, tesorero, vocales, se reúnen una o más veces al año y suelen editar unas conclusiones o boletines, que intentan coincidir en todo y aplaudir, las conclusiones previas emanadas de comités europeos o americanos.
Y de este preámbulo extraigo mi primera recomendación para el futuro de la Nutrición Enteral: intentar reducir las sociedades y con ellas el esfuerzo económico y pérdida de tiempo, que conllevan y centralizarlo en un número más reducido, dedicando esfuerzo, euros y tiempo en crear líneas de investigación propias de nuestro país que puedan responder los interrogantes de las necesidades actuales de esta faceta de la medicina.
Otro punto a considerar es la tendencia apreciada a lo largo de los últimos años, de potenciación de la Alimentación Enteral a Domicilio, por infusión oral o por sonda nasogástrica o PEG, de innegables ventajas para el enfermo y para la más que recortada economía de nuestros hospitales; sería conveniente potenciar este tipode alimentación.
A tenor de los resultados y de la proliferación de las casas comerciales que los suministran, podemos asegurar que la nutrición enteral goza de buena salud, y con perspectivas buenas de desarrollo en un futuro.
Perspectivas y expectativas de desarrollo con ampliación a nuevos productos además de los existentes que ya se han tratado en este curso. Estas expectativas más que recomendaciones, estarían centradas en la composición de las futuras fórmulas.
- E n Nutrición Enteral (EN) para recién nacidos, inmaduros, con riesgo de sepsis, faltaría una fórmula con baja o normal osmolaridad, con un aporte de poliinsaturados de larga cadena (PUFA), nucleótidos, hierro,zinc, Ca, con un aporte de MCT, dextrinomaltosa y la proteína extensamente hidrolizada o bien a base de aminoácidos libres.
- Para lactantes y niños afectos de alergia a las proteínas de leche de vaca, o también a otros alèrgenos alimentarios una formula con proteína de vaca hidrolizada y adicionada de probióticos, por el estímulo de las TH1 que ejercen en detrimento de las Th2 vinculadas a la producción de IgE, en un intento de acortar la duración de la alergia.
- En el Intestino corto, una fórmula similar con un aporte especial de ácido fólico, vitamina B12 (por carecer muchos de ellos de ileon distal).
- E n inmunodeprimdos, garantizar con la fórmula un aporte de nucleótidos, Zinc, hierro, lactoferrina humana; se habría de crear líneas de trabajo en nuestro país para conseguir lactoferrina humana; en su defecto usar la bovina de la que es fácil disponer; garantizar el aporte de PUFA, vitamina A (estimulante de la inmunidad celular) y otras vitaminas liposolubles. Adición de probióticos, factores de crecimiento, poliaminas.
- En afectos de Fibrosis Quística (FQ) formula enteral de aproximadamente 1 ml = 1 kcal, con PUFA, monoinsaturados (MIS), parte de MCT, con las proteínas parcialmente hidrolizadas por la disminución de la actividad enzimtica pancreática, con alfa lactoalbúmina y triptofano. La fuente hidrocarbonada debería ser lactosa más polímeros de glucosa por la baja actividad amilolítica pancreática de la FQ, como demostramos y publicamos en JPGN, además de un aporte generoso de vitaminas liposolubles, y cierta cantidad de colesterol; en la FQ la cifra de colesterol está en un 90% de casos baja, siendo importante para la formación de hormonas sexuales, formación de membranas, formación de bilis.
- Para la obesidad una fórmula líquida con un aporte calórico bajo, 35 - 50 kcal por 100 ml, baja en grasas, con ácido gama-linolénico, con lactosa, aporte proteico normal, entre una formula de continuación y leche de vaca, con fibra soluble con capacidad hidratante para aumentar la sensación de repleción; aporte adecuado de vitaminas, minerales y oligoelementos.
- En la Enfermedad Inflamatoria Intestinal una fórmula monomérica con aminoàcidos libres u oligopéptidos de bajo peso molecular, con probióticos, transforming growth factor beta, en un intento de frenar la producción de Tumor Necrosis Factor.

ABSTRACTS SEINAP 04
1. LACTOSE INTOLERANCE. INVEST NUTR ALIM PEDIATR (Rev on-line) 2004; 2.
#03. http:// www.seinap.org M. Moya y M. Juste. Hospital Universitario San Juan. Alicante. SpainThere are two main types of lactase deficiency in man. In primary deficiency the proteic gene expression fails. It is manifested through three different clinical situations: a) Deficit related to development, this is the case of the extreme preterms. b) Congenital lactase deficiency so rare that only merits this mention. c) Late onset hypolactasia or adult type which is the best known and studied one. This is not considered as a disease because when considering the population as a whole only a minority keeps the lactase activity of the infant period up to adulthood. Despite late onset hypolactasia term, its beginning sometimes comes in the paediatric years, specially in lactose-intolerant populations. The fact of an adequate tolerance of sucrose and maltose points to the absence of a generalised mucosal lesion. In Europe (except Scandinavian areas) and in the U.S.A. and Canada the low levels of lactase activity are not apparent before five years of age. To such an extent that if a child less than this age shows a lactose maldigestion (BH2 >20 ppm) one should always consider the possibility of mucosal damage. Secondary lactose deficiency comes after a lesion of the small intestine mucosa and can be acute or chronic. In the acute case the optical morphology of the enterocyte is not altered and the usual consequence is a temporary intolerance of the disaccharides (very seldom monosaccharides). This is always in close relationship to the intensity of the diarrhoeal episode and above all with the fact of a malnutrition status. Other rarer causes can be a blind loop or bacterial overgrowth. Chronic secondary forms are related to untreated celiac disease, cow's milk protein intolerance, lambliasis, prolonged diarrhoea or anti-cancer treatment. These secondary deficits are offen over valued and over treated in the normal medical care of children.1. Breath Hydrogen Test (BH2).This is the most widely used method to detect carbohydrate intolerances. Malabsorbed carbohydrate in the small intestine will later be fermented by colonic bacteria releasing hydrogen, CO2 and methane. A proportion of these gases is absorbed and breathed out: 15%-20% of the H2 generated in the colon. In the case of lactose, after a fasting period the basal BH2 is measured, followed by lactose water solution (never milk) of 1-2 g/kg (< 50g) and finally the breathed out hydrogen is measured. We consider figures to be abnormal if they are greater than 10-20 ppm over the basal measurement. This allows lactose absorption to be measured indirectly with a high sensitivity rather than invasively.Clinical assessment.Symptoms of bloating, swelling, flatulence and diarrhoea, 3-4 hours after having a glass of milk (approx. 12 g of lactose) are better identified by adults than children. The problem arises when through the BH2
screening high values are found in individuals with no symptoms. This can be due to different personal thresholds for these symptoms, to the remaining lactase activity but above all for the lactose colonic management. This last factor makes adult tolerance from 0.25-1.0 litres of milk possible. Nevertheless there are no significant differences in these patients when they have taken 200 ml. of milk with or without lactose when studied under a double blind challenge. This fact underlines the importance of the lactose intolerance self consideration, furthermore in paediatric ages the important role of intolerance 'by proxy' is increasingly common. Lactose maldigestion and recurrent abdominal pain (RAP) has been widely evaluated without a clear association between both of them. In thirteen cases of pure RAP studied by us, not only the espiratory peak median has been found normal in all of them but also the CI 95% remains below the 20 ppm. It is also worth noting that the area under the curve in patients with mucosal damage or other important lesions, values which lay outside of CI 95%. To conclude it is necessary to refer to the dietary treatment of acute diarrhoea (Kind & Duggan, 2003) in which it is clear to maintain breast feeding without restriction and in the case of bottle fed infants they should continue with the same standard formula once the oral rehydration period has been accomplished. There is no indication that the use of lactose-free formulas carries out any therapeutic advantage. In children refined sugar should be avoided and caloric intake should be normalised the sooner the better. 2. FEEDING FORMULAS. WHAT’S NEW ABOUT THEM THAT IS REALLY USEFUL?. INVEST NUTR ALIM PEDIATR (REV ON-LINE) 2004; 2. #04. HTTP://WWW.SEINAP.ORG Angel Ballabriga.

Department of Pediatrics, Autonomous University, Barcelona.Summary. At present there is an extraordinarily high and varied number of feeding formulas on sale in our country that are orientated towards the different stages of alimentation in infancy, both for the normal child and for those that present more or less specific problems susceptible to treatment by industrially modified foods. At first sight then it would seem that the industry, both national and foreign, that is dedicated to the feeding and nutrition of the infant population has consolidated a solid basis in that which refers to nutritional research, relation with pediatricians, marketing, distribution of products and scientific collaboration. When I was asked to participate in this session and faced with a title that seemed to me to be rather provocative, my first intention was to smooth it over but afterwards I have changed my mind about this because I believe that it is a question that perhaps is needful of some deeper thought. On the other hand, to make a detailed revision in order to answer objectively and with the least possible margin of error the question as to what is new that is really useful in the feeding formulas on the market today, would be a task that would require not only all the time that we dispose of in this session but also two or three more days together with the collaboration of other colleagues that are experts on the different combinations concerning this matter. For this reason it seems more logical to me to limit myself to presenting some comments about the employment and quantification of proteins in the formulas for normal infants, given that other colleagues in this session will occupy themselves with the concrete aspects of carbohydrates and fats, so that afterwards the subject can be globally presented for a joint discussion. During the seventh meeting of the ESPGAN Society in Verona in 1974, it was decided to create a Committee on Nutrition for the consideration of standards and regulation of infant feeding, committee of which I had the honour of being a member of for 8 years. A first document was redacted on the composition of the formulas that were called adapted that was discussed in Weimar in 1976 in the ninth meeting of the society and which was later published in 1977 as supplement 262 in Acta Paediatrica Scandinavica. Regarding proteins, the recommendation was of 1.8-2.8/100kcal, that is 1.2-1.9/100ml and the document was based on the personal experience of the 10 committee members and 109 articles published up to that moment concerning the matter that the committee had considered useful. From this very moment the European industry made a wide echo of these recommendations. In a second document (Acta Paed.Scand. suppl.287) published in 1981, recommendations were quoted for the composition of follow up formulas and complementary feeding, the protein intake was established at 3.0-5.5g/100kcal. Some years later (1990) the maximum limit was reduced to 4.5g/100kcal, given that in European countries and in accordance with local habits of that time, the protein content of complementary feeding was traditionally high. Over the following years trials have been carried out with adapted formulas in which the protein intake has been reduced to 1.8g/kg/day, using modified proteins in the sense of a predominant addition of whey proteins or partially hydrolysed whey proteins, or with formulas in which the presence of threonine-rich macropeptide has been eliminated and which is characteristic of sweet whey and responsible for the hyperthreoninemia observed with the use of some formulas. Enriching with a-lactalbumin supposes the addition of tryptophan intake which is the limiting aminoacid in low protein formulas. Likewise, matters are discussed in relation to plasma aminoacids and the role played by bacteria of the colon using ureic nitrogen for synthetising available aminoacids. Finally, the role of dietetic regulation expressed by genes in the developing intestinal epithelium is commented on. 3. THE IMPORTANCE OF LIPIDS IN NUTRITION. INVEST NUTR ALIM PEDIATR (REV ON-
LINE) 2004; 2. #05. HTTP:// WWW.SEINAP.ORG H. BöhlesKlinik für Kinderheilkunde, Johann Wolfgang Goethe-University Frankfurt/Main, GermanyModern knowledge about lipids is opening the understanding beyond their use as a mere high energy source. A predominance of fat oxidation leads to an increased ketogenesis resulting in a lowering of the RQ. Both effects can be used as a ketogenic diet in the treatment of epilepsy and selected inborn errors of metabolism such as glut-1 deficiency as well as in chronic lung disease, taking advantage of a lowered CO2 production. However, it is the improved knowledge about individual fatty acids that forms the basis of the nutritional use of lipids in pathophysiologically defined situations. Fatty acids of the w-6 family mainly represented by arachidonic acid (AA) (20:4 w-6) emphasize inflammatory mechanisms on the basis of prostanoid synthesis, whereas those of the w-3 family have anti-inflammatory potential. This leads to distinct nutritional concepts in patients with i.e. inflammation dominated diseases like Crohn´s

disease, asthma or cystic fibrosis. Recently special interest has focused on the importance of individual fatty acids, mainly polyunsaturated long chain fatty acids of the w-3 family such as eicosapentaenoic acid (EPA) (20:5 w-3) and docosahexaenoic acid (DHA) (22:6 w-3) and of the w-6 family, mainly arachidonic acid (AA) (20:4 w-6). The understanding of the importance of DHA starts in late pregnancy, when it is realized that DHA is enriched in the fetus by means of a special placental fatty acid carrier system. This particular supported supply is postnatally continued when the child is breast fed. About 0.6 % of total fatty acids in maternal milk are represented by DHA. DHA contributes a great deal to the myelination of the central nervous system. An adequate supply is therefore extremely important during the first two years of life. Breast-fed infants and infants fed formulas supplemented with DHA and AA have better neurofunctional outcomes. Because of this, formulas are now fortified with DHA and AA. Low DHA concentrations have been described in a large variety of diseases. Among them are: Phenylketonuria (PKU): The dietary treatment of this disease largely precludes the major source of DHA and AA. Patients must rely on the endogenous synthesis from their precursors like a-linolenic acid (18:3 w-3), which also is often suboptimal. A successful dietary treatment of PKU may therefore result in an iatrogenic decrease in the circulating DHA pools. The functional consequences of fatty acid supplementation are still under debate. As human milk is a rich source of preformed long chain polyunsaturated fatty acids, it is tempting to emphasize breast feeding in PKU-patients. Pregnant women with PKU and poorly compliant patients with the condition also might benefit from preformed fatty acid supplementation. Cystic fibrosis (CF): A fatty acid imbalance, i.e., elevated AA and low DHA, was demonstrated in a CF-mouse model. Oral administration of high doses of DHA not only corrected the membrane lipid imbalance but also reversed the signs of CF in the affected mice. Improvement of pulmonary function has been observed in CF-patients after 6-weeks to 8-months treatment with w-3 long chain polyunsaturated fatty acids, including both EPA and DHA. Attention-deficit/hyperactivity disorder (ADHD): Its etiology is poorly understood. In affected children low DHA concentrations in plasma and erythrocyte phospholipids have been observed. It is the objective of present investigation to study the influence of DHA-supplementation on the clinical symptoms of ADHD patients. Peroxisomal disorders: Patients with generalized peroxisomal disorders have profound brain deficiency of DHA. Consequently the use of DHA in patients with these disorders is common. With treatment clinical improvement has been reported. It has been speculated that DHA acts at the level of the cellular membrane of the oligodentrocyte or neuron.Modern nutrition considers the importance of lipids beyond their effects of high caloric density with the intention to influence membrane function, signal transduction and mechanisms and intensity of inflammatory reactions. 4. STUDY OF THE POLYUNSATURATED AND TRANS FATTY ACID CONTENT IN DIFFERENT PEDIATRIC POPULATIONS: THEIR ROLE IN NUTRITION AND PREVENTION OF CARDIOVASCULAR DISEASE. INVEST NUTR ALIM PEDIATR (REV ON-LINE) 2004; 2. #06. HTTP:// WWW.SEINAP.ORG Pablo Sanjurjo, Luis Aldámiz-Echevarría and José Angel PrietoObjective: the valoration of the relationship between the polyunsaturated and trans fatty acids content in adipose tissue and muscle in children, and the risk factors of cardiovascular disease, especially insuline peripheral resistance.Design: transversal study, with a length of three years.Location: Departamento de Pediatría-Unidad de Metabolismo Pediátrico, Hospital de CrucesSubjects: 120 healthy children of both sexes undergoing elective surgery, and divided in four age groups (0-2, 2-5, 5-10 and >10 years).Determinations: somatometry. Fatty acid composition of skeletal muscle membrane phospholipids and adipose tissue, basal levels of glucose, insuline and lipidic profile.
Results and conclusions
Both glucose and insuline levels, and HOMA index increase through the four pediatric ages studied (1.71±0.84; 1.61±0.81; 2.68±1.67 and 3.77±1.58). However, the results are statistically significant only between the two last groups (5-10 years and >10 years), and the two first groups (0-2 and 2-5 years). Although a physiological resistance to insuline is reportedly possible at puberty (group 4, more than 10 years old), it is worrying that it is already defined at younger ages (5-10 years).
The study of fatty acid composition of muscle membrane phospholipids has intrinsically the value of reporting reference values for children at different ages, which had not been previously reported in bibliography (there is just a study performed at breastfeeding period). It is worth mentioning the continuous decrease of oleic acid percentage (9.11±2.23; 8.93±1.79; 8.20±1.23 and 8.12±1.34), and the

increase of linoleic acid (18.14±5.01; 24.0±3.71; 25.61±3.63 and 27.47±3.66), and trans fat (0.27±0.11; 0.31±0.15; 0.37±0.13 and 0.35±0.14), which confirms at tissue level the pediatric loss of the Mediterranean diet.
The analysis of the fatty acids in adipose tissue has the utility of reporting their reference values for infants (there are just partial data obtained by our research group in 1987). It is worth pointing out the increase of linoleic acid percentage with age (12.38±2.16; 14.26±3.32; 15.0±2.96 and 14.44±2.75), and its metabolite, arachidonic acid (0.27±0.13; 0.20±0.04; 0.24±0.1 and 0.29±0.08).
These data, along with the results obtained for the muscle membrane phospholipids, confirm the abandoning of Meditarranean diet by children, as well as the excesive consumption of linoleic acid. 5. GHRELIN AND ADIPONECTIN: THEIR ROLE IN CHILDHOOD OBESITY. INVEST NUTR
ALIM PEDIATR (REV ON-LINE) 2004; 2. #07. HTTP:// WWW.SEINAP.ORG Ángel Gil1, Mercedes Gil2 y Ramón Cañete2
1Department of Biochemistry and Molecular Biology, University of Granada, Granada, and Unit of Paediatric Endocrinology, Department of Paediatrics, Reina Sofia Universitary Hospital, Cordoba
The regulation of nutrient intake is a key process in the maintenance of body weight. Ghrelin is a peptide produced in the stomach whose main functions are to be the natural endogenous ligand for the growth hormone secretagoge receptors and to regulate the energy balance. The most important factors promoting ghrelin secretion are hypoglicemia, leptinemia and fasting, whereas food intake and hyperglicemia inhibit it. The nutritional status appears to be a key determinant in establishing plasma ghrelin concentrations, being increased under negative balance conditions and increased under positive energy balance. In fact, plasma ghrelin levels are strictly dependent on recent food intake. However, whether insulin or glucose is the regulator of ghrelin secretion remains to be ascertained. Moreover, it has been suggested that mutations or alterations in the control of ghrelin secretion might be involved in the aetiology of human obesity.
In a recent study carried out by our research group in prepubertal children, they showed a specific postprandial ghrelin course, different than that exhibited by controls, characterised by a quick return to fasting levels. In addition, ghrelin plasma levels were associated mainly with glucose, which suggests that glucose is a key factor in the regulation of ghrelin secretion in childhood. Moreover, the rapid return of ghrelin to fasting levels provides a potential explanation for a bigger intake of food as observed in obese children.
Although obesity is frequently accompanied by insulin resistance, diabetes, metabolic syndrome and cardiovascular diseases, the molecular basis for the link between obesity and those diseases has not yet been clarified. Adiponectin, or Acrp30, is an exclusive adipocyte-derived citokine, which represents the most abundant transcript for adipose tissue, accounting for 0.01% of total plasma protein. It has been reported that adiponectin appears to play an important role in the regulation of energy homeostasis and insulin sensitivity, and it may have putative antinflammatory and anti-atherogenic properties. Adiponectin expression is reduced in obese individuals and insulin and other negative modulators of insulin action, namely TNF-α, repress the expression of adiponectin. In addition, a number of adiponectin polymorphisms have been associated to an increased risk of obesity, diabetes type 2, insulin resistance and dislipidemia. These subjects show very low levels of plasma adiponectin.
The molecular mechanism by which adiponectin improves insulin sensitivity seems to be related to an increase in fatty acid oxidation, as well as a reduction in hepatic gluconeogénesis and an increase in glucose uptake by skeletal muscle. These effects are mediated by the interaction with muscle and hepatic receptors through activation of AMP kinase, the cellular “fuel gauge”, which in turn inhibits acetyl CoA carboxylase and increases fatty acid β-oxidation. In our study, adiponectin concentrations were decreased in obese children as compared to controls, without changes during the postprandial period. Likewise, the levels of this hormone were negatively correlated with those of insulin, HOMA and leptin, and negatively with plasma tryglicerides and other markers of cardiovascular disease, which suggest the important role of adiponectin in the regulation of insulin resistance since early ages. 6. GENETIC PATTERN OF LACTOSE MALABSORPTION IN GALICIA. INVEST NUTR ALIM PEDIATR (Rev on-line) 2004; 2. #08. http:// www.seinap.org R. Leis, A. Tocoian, A. Martínez, A. Novo, R. Tojo
Unidad de Investigación en Nutrición y Desarrollo Humano de Galicia. Cátedra Novartis Medical Nutrition-Universidad de Santiago de Compostela de Nutrición Clínica Pediátrica. Departamento de Pediatría. Hospital Clínico Universitario de Santiago. USC. España.The late lactase deficiency or the primary adult-type hypolactasia or the primary lactase non persistence is the most common type of genetically determined disaccharidase deficiency. It is transmitted with autosomal recessive inheritance, whilst its persistence is transmitted with autosomal dominant inheritance. In an important percentage of the affect individuals, the lactose intake is followed by a gastrointestinal clinical symptomatology like diarrhoea, abdominal pain, flatulence, nausea or vomits, which entails a rejection or the lack of intake of this food containing lactose, milk and milk-based products.The prevalence of the primary adult-type hypolactasia diverges a lot depending on the region, showing a positive geographical gradient North-South. Thus, a prevalence of a 2-3% is observed in Scandinavia and until a 70% in Sicily. Studies carried out by our task force in Galicia during the 90’s of the 20th century prove that a 38.4% of the population shows an alteration in the lactose metabolism after making the hydrogen breath test post-overload with 2g of lactose/kg weight at 20% inwater(<50g). Moreover, the loss of enough lactase activity which brings about lactose intolerance begins from 6 years old. The prevalence is subsequently maintained in similar percentages during the whole life cycle. These figures correspond to the fact that our region is geographically placed in Southern Europe, which would favour the high prevalence of enzymatic deficiency. But on the other hand, this region is traditionally a cattle-breeding area, with high levels of precipitation, so there are few hours of sunlight. Thus, vitamin D levels are relatively low and a higher calcium intake is necessary. This would favour the enzymatic activity persistence.ObjectiveRecent studies in Finland show the prevalence of two polymorphisms correlated to lactose malabsorption, the C/T-13910 and G/A-22018. That is why we considered interesting to determine the prevalence of lactose malabsorption in children who come to gastroenterology consultation in our department suffering from abdominal pain, diarrhoea and/or other gastrointestinal symptoms. We consider interesting to determine the hydrogen production and the symptoms shown during the test depending on the diagnosis, to know the absorption and resistance to different lactose doses administered in different ways to formulate adequate nutritional recommendations, to determine the polymorphisms correlated to malabsorption in our population, to study the correlations among polymorphisms, diagnosis, hydrogen production and symptomatology, and finally to study the possible use of a genetic test for lactose malabsorption early diagnosis in Galician children. Material and methodBetween January and July 2004, 363 children were examined (42,1% males and 57,9% females), with an age range between 2 and 15 years old. The sample was stratified in 3 groups depending on the reason for the consultation: A-251 children showing abdominal pain, B-20 who presented diarrhoea and C-33 who showed abdominal pain and diarrhoea. Breath hydrogen was measured after a lactose overload (2g/kg lactose weight, no more than 50g) and the gastrointestinal symptoms were recorded during the test. 135 of the examined children were extracted a peripheral blood sample and from the leukocyte DNA, the 2 fragments included in each polymorphism were amplified with PCR. Later, the PCR products sequencing was made. In collaboration with the Genetic Unit of our Hospital, the technique to make the genotype using the Sequenom Platform® has began (particle mass Spectrophotometry), in order to detect polymorphisms C/T-13910 and G/A-22018. ResultsThe incidence of lactose metabolism alterations after the lactose overload was of 28,4%, from which: 24% were bad absorbers( H2>20ppm) and 4,4% deficient absorbers (H2: >10ppm and <20ppm). As for the 252 absorbers (H2<10ppm), most of them (93,8%) were lactose tolerant (with no symptoms during the test) and only 6,2% were intolerant (with symptoms during the test). Taking into account the 89 bad absorber children, 68,3% were tolerant and 31,7% intolerant. The main symptoms shown during the test were: abdominal pain both for absorbers (4,3%) and for bad absorbers (21,3%), followed by diarrhoea, which happens more frequently in bad absorbers (9%) than in absorbers (1,2%). As for group A, a 73,3% of the examined subjects showed lactose absorption, a 23,1% malabsorption and a 3,5% deficient absorption. In group B, a 70% showed lactose absorption, a 20% malabsorption and a 10% deficient absorption. In group C, the 69,7% of the children showed absorption, 27,3% malabsorption and 3% deficient absorption.The lactose malabsorption prevalence found in our study is similar to other prevalences found in field studies inside our region. Comparing the 3 groups, more bad absorbers were found among those children showing abdominal pain and diarrhoea as the main reason for consultation. The results of the genotype and the finding or not of polymorphisms will allow us to study their possible correlations to the clinical

expression of lactose malabsorption and to establish a genetic test which permits us to make a diagnosis and an optimal nutritional therapy. BibliographyBersaglieri T, Sabeti PC, Patterson N, Vanderploeg T, Schaffner SF, Drake JA et al. Genetic signatures of strong recent positive selection at the lactase gene. Am J Hum Genet 2004; 74 (6): 1111-20.Enattah Sabri N, Sabri T, Terwilliger J, Peltonen L, Järvelä I. Identification of a variant associated with adult-type hypolactasia. Nat Genet 2002; 30: 233-237.Harvey CB, Hollox EJ, Poulter M, Wang Y, Rossi M, Auricchio S et al. Lactase haplotype frequencies in Caucasians: associations with lactase persistence/non-persistence polymorphism. Ann Hum Genet 1998; 62: 215-223.Leis R, Tojo R, Pavón P, Douwes A. Prevalence of lactose malabsorption in Galicia. J. Pediatr. Gastroenter. Nutr. 1997; 25: 296-300.Leis R, Tocoian A, Martínez A, Novo A, Villar H, Zimmo S, Tojo R. Sintomatología gastrointestinal sugestiva de malabsorción a la lactosa en niños. Confirmación mediante el test de hidrógeno espirado. Pediatrika 2004; 24 (5): 40.Mulcare CA, Weale ME, Jones AL, Connell B, Zeitlyn D, Tarekegn A et al. The T allele of a single-nucleotide polymorphism 13.9kb upstream of the lactase gene (LCT) (C-13.9kb T) does not predict or cause the lactase-persistence phenotype in Africans. Am J Hum Genet 2004; 74 (6): 1102-10.Poulter M, Hollox E, Harvey CB, Mulcare C, Peuhkuri K, Kajander K et al. The causal element for the lactase persistence/non-persistence polymorphism is located Mb region of linkage disequilibrium in Europeans. Ann Hum Genet 2003; 67 (Pt 4): 298-311. 7. BIOCHEMICAL PARAMETERS AND NUTRITIONAL STATUS. INVEST NUTR ALIM
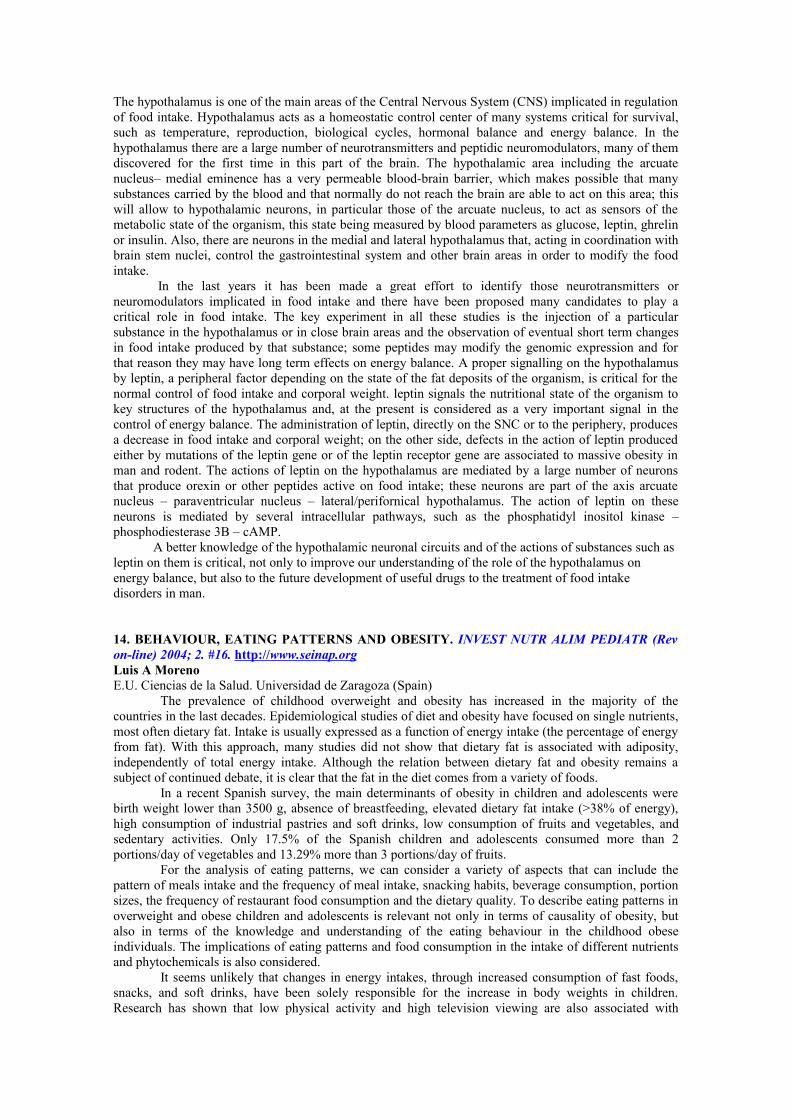
PEDIATR (Rev on-line) 2004; 2. #09. http:// www.seinap.org Ros Mar L, Guallar Labrador A, Ros Arnal I, Sáenz Moreno I.“Miguel Servet” Hospital, Zaragoza, Spain.In the valuation of the state of children's nutrition, multiple methods are used: clinical, antropometric and biochemical. However it has been always difficult to select the most suitable parameters in each case.The aim of this study was to clarify the relationship between normally used biochemical parameters and certain nutritional situations.Patients and method: 896 children, 463 women and 433 males were studied Their age was between 2 and a half years and 18 years old. The patients were included in three groups: 1) malnourished (354) which were under –2 BMI SD, 2) control group (426) among - 1 and + 1 SD, and 3) obese (116) upper + 2 BMI DS. The Andrea Prader charts made from Aragon children were used as reference measures. The serum concentrations of cholesterol, triglycerides, iron, ferritin, copper, zinc, albumin, prealbumin, IGF-1, IGFBP-3, leptin, folic acid and vitamin B12 were carried out The final results are expressed in the chart below:
P<0,001
Malnourished Control ObesesMalnourVs control
Control Vs obeses
MalnourVs obeses
Patients 354 426 116
Age 6,69 ± 3,65 7,28 ± 3,84 7,24 ± 3,77 no no no
BMI SD -2,96 ± 0,78 -0,14 ± 0,58 3,37 ± 1,26 yes yes yes
Cholesterol 173,79 ± 31,22 169,64 ± 29,8 174,62 ± 32,88 no no no
Triglycerides 55,05 ± 21,77 53,79 ± 20,06 65,02 ± 45,55 no yes yes
Iron 78,27 ± 32,45 81,78 ± 33,25 76,52 ± 31,57 no no no
Ferritin 28,49 ± 18,93 30,58 ± 19,75 31,09 ± 26,26 no no no
Copper 131,82 ± 30,85 132,12 ± 29,44 135,04 ± 26,81 no no no
Zinc 95,94 ± 16,12 95,83 ± 16,37 99,13 ± 15,14 no no no
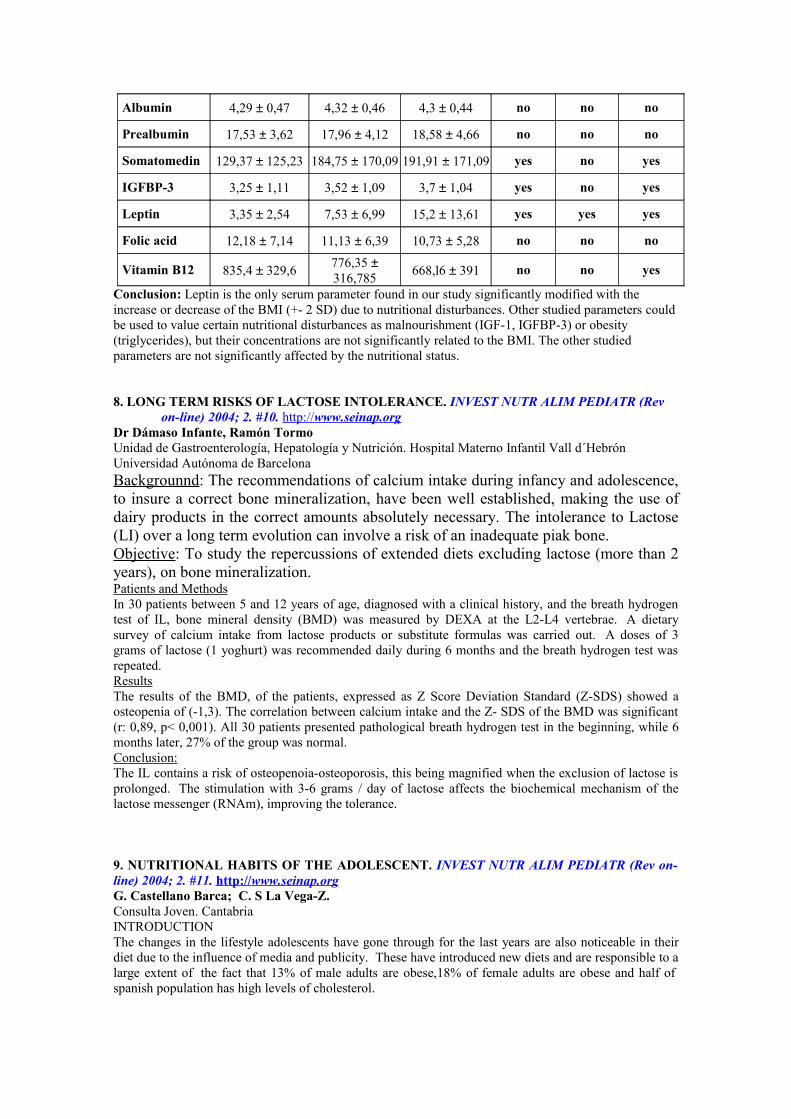
Albumin 4,29 ± 0,47 4,32 ± 0,46 4,3 ± 0,44 no no no
Prealbumin 17,53 ± 3,62 17,96 ± 4,12 18,58 ± 4,66 no no no
Somatomedin 129,37 ± 125,23 184,75 ± 170,09 191,91 ± 171,09 yes no yes
IGFBP-3 3,25 ± 1,11 3,52 ± 1,09 3,7 ± 1,04 yes no yes
Leptin 3,35 ± 2,54 7,53 ± 6,99 15,2 ± 13,61 yes yes yes
Folic acid 12,18 ± 7,14 11,13 ± 6,39 10,73 ± 5,28 no no no
Vitamin B12 835,4 ± 329,6776,35 ± 316,785
668,l6 ± 391 no no yes
Conclusion: Leptin is the only serum parameter found in our study significantly modified with the increase or decrease of the BMI (+- 2 SD) due to nutritional disturbances. Other studied parameters could be used to value certain nutritional disturbances as malnourishment (IGF-1, IGFBP-3) or obesity (triglycerides), but their concentrations are not significantly related to the BMI. The other studied parameters are not significantly affected by the nutritional status. 8. LONG TERM RISKS OF LACTOSE INTOLERANCE. INVEST NUTR ALIM PEDIATR (Rev
on-line) 2004; 2. #10. http:// www.seinap.org Dr Dámaso Infante, Ramón TormoUnidad de Gastroenterología, Hepatología y Nutrición. Hospital Materno Infantil Vall d´HebrónUniversidad Autónoma de BarcelonaBackgrounnd: The recommendations of calcium intake during infancy and adolescence, to insure a correct bone mineralization, have been well established, making the use of dairy products in the correct amounts absolutely necessary. The intolerance to Lactose (LI) over a long term evolution can involve a risk of an inadequate piak bone. Objective: To study the repercussions of extended diets excluding lactose (more than 2 years), on bone mineralization.Patients and MethodsIn 30 patients between 5 and 12 years of age, diagnosed with a clinical history, and the breath hydrogen test of IL, bone mineral density (BMD) was measured by DEXA at the L2-L4 vertebrae. A dietary survey of calcium intake from lactose products or substitute formulas was carried out. A doses of 3 grams of lactose (1 yoghurt) was recommended daily during 6 months and the breath hydrogen test was repeated. ResultsThe results of the BMD, of the patients, expressed as Z Score Deviation Standard (Z-SDS) showed a osteopenia of (-1,3). The correlation between calcium intake and the Z- SDS of the BMD was significant (r: 0,89, p< 0,001). All 30 patients presented pathological breath hydrogen test in the beginning, while 6 months later, 27% of the group was normal. Conclusion:The IL contains a risk of osteopenoia-osteoporosis, this being magnified when the exclusion of lactose is prolonged. The stimulation with 3-6 grams / day of lactose affects the biochemical mechanism of the lactose messenger (RNAm), improving the tolerance. 9. NUTRITIONAL HABITS OF THE ADOLESCENT. INVEST NUTR ALIM PEDIATR (Rev on-line) 2004; 2. #11. http:// www.seinap.org G. Castellano Barca; C. S La Vega-Z. Consulta Joven. CantabriaINTRODUCTIONThe changes in the lifestyle adolescents have gone through for the last years are also noticeable in their diet due to the influence of media and publicity. These have introduced new diets and are responsible to a large extent of the fact that 13% of male adults are obese,18% of female adults are obese and half of spanish population has high levels of cholesterol.
We believe that a balanced diet is the one that provides 50%-55% of carbohydrate, 30%-35% of lipids, and 15% of proteins. Thus, the intake should range between 2.500 and 3.000 calories for males and between 2.200 and 2.500 calories for females. Let´s remind that throughout puberty 25% of adult height is gained and 40%-50% of definitive weight, muscular mass doubles and skeletal mass increases 50%.AUXOLOGYFor the last decades the height and weight of spanish adolescents is nearly at the same level than european ´s due to a better diet even though there are other factors. Around the middle of ninenteenth century, northamerican adolescents were beetween three and nine centimetres taller than the population of northern and western Europe. At present thanks to a better diet, europeans are taller than north american, they continue growing and are not affected by a epidemic obesity.According to PAIDOS survey of 1985, 4,9% of childrens aged 6 to 12 were obese. KID survey of 1998-2000 pointed out that, 13% of the population aged 2 to 24 were obese and according to González Montero de Espinosa and Marrodán Serrano survey of 1998/2000, 19,46% of male adolescents presented weight excess and the percentage for females reached 14,76%. 4,87% of males were obese and the percentage for females reached 2,87%.On the other hand throughout the twentieth century, females are 20,9cms taller and males 23,8cms as long as secular acceleration of the height is concerned. Besides from the end of the ninenteenth century to the present the age when the shoot up takes place has come early at the average of 0,2 years per decade.Shall we end this chapter recalling that 24% of male adolescents and 53% of female adolescents are dissatisfied with their corporal appearance and would like to be slimmer.PRESENT DAY DIETThe consumption of proteins by Spanish adolescents doubles the real needs, mainly because of meat (45% beef, 30% pork and 25% chicken).69% of males present a shortage of carbohydrates and 56% of females too. Besides, there is a slight excess of fat. The consumption of eggs, pulse, vegetables and fruit is low and downward trend.According to González Montero De Espinosa and Marrodán Serrano, the levels of vitamins B12 and A are high. For the complex B, its levels are on the limit. There is a lack of vitamin D palliated by the sun and a clear shortage of vitamin B mainly in females. They do not satisfy 25% of their needs. There is a slight lack of calcium, iron is at the limit and males over 18 and all females are short of iodine. Levels for P, Mg and Zn are normal The intake is slightly high in males from 12 to 20 and slightly low for females.45%-50% drink water, 44% soft drinks or colas and 5% juices. 3% of the males aged 14 to 20 are on a diet and 12% of females of the same age. 12%-15% of males aged 18 do not have breakfast and 10% of adolescents aged 14 to 18 neither.CONCLUSIONSWe must work to achieve that yougnsters do not lose the standards of proper diet . Wrong diets and fast food must be avoided as well as any food of little nutritional value. The increasing consumption of soft drinks must be corrected. Breakfast must represent 20% of the intake, morning snack 10%, lunch 35%, afternoon snack 10 and dinner 25%.Let´s forget the eternal lamentations about the wrong diet of adolescents. We shall come into action by means of an efficient , coordinated and long term health education. SEINAP. ORG. BOL E NUTR ALM PEDIATR 2004(2) #09 10. CHANGES IN LIPID PROFILE IN EGG YOLK ACCORDING TO BIRD FEEDING TYPE.INVEST NUTR ALIM PEDIATR (Rev on-line) 2004; 2. #12. http:// www.seinap.org E. Cortés; M. Moya; J. LugoPediatric Departament. Miguel Hernández University. San Juan Hospital . AlicanteIntroduction. Egg is a food with a high nutritive value, due to its good taste, high protein content (white), easy digestion and an appropiate proportion of amino acids, good content of A,B.B12, D and E vitamins, minerals, O, Se Fe Y and Zn.Yolk is rich in phospholipids and it has a good saturated / unsaturated fatty acid rate. Because of his high cholesterol content (>200 mg/yolk) a restrictive tendency has been developed. Trying to compensate this problem, eggs with docosahexaenoic acid (DHA) added have been marketed and differences in the lipid profile have been studied (1). In this sense different complements to the fodder used in poultry farms has been tried attempting to produce either, lower cholesterol or DHA enriched eggs (2). The aim of the present work is to determine the lipid profile of the usual commercial and household hens produced eggs.Material and methods. The lipid composition of yolk of shopping eggs (n=15) and household eggs (n=15), with a total egg weight of 65.2 g (SD 6.0) and 55.3g (SD10.5) (p<0.005, Kruskal-Wallis test) and a yolk weight of 18.8g (SD 3.1) and 14.5g (3.5) (p<0.005) respectively. Analyzed parameters were:
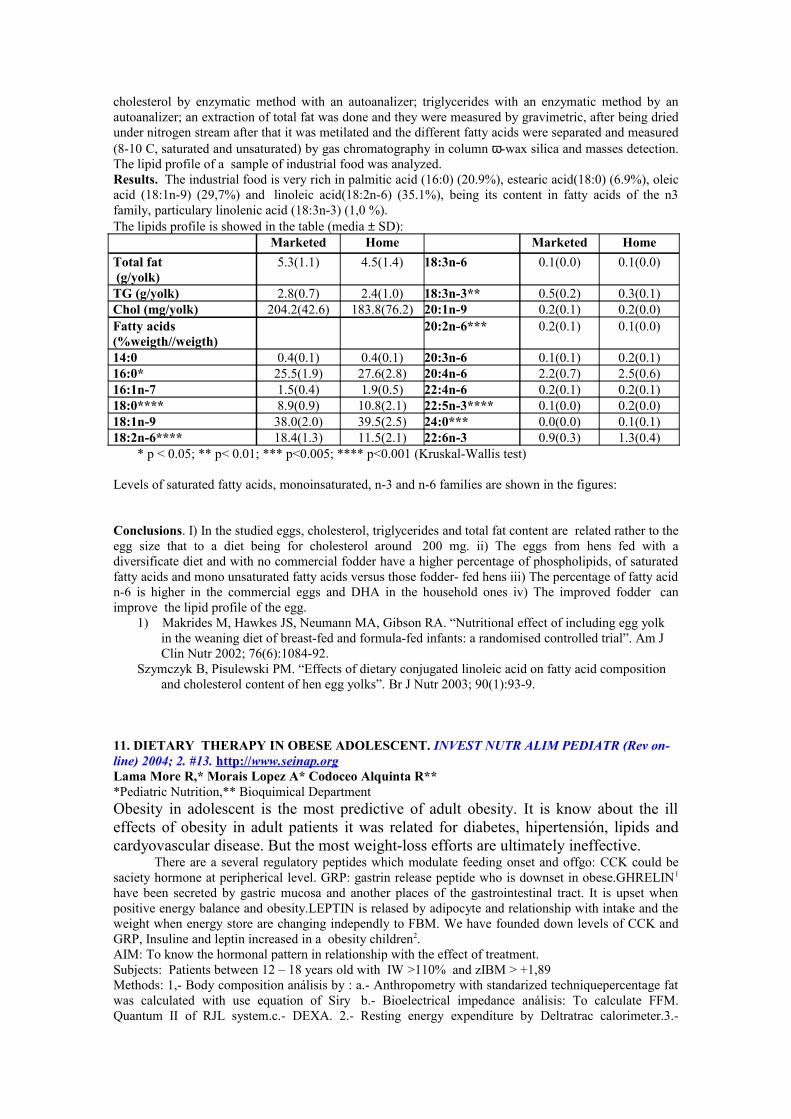
cholesterol by enzymatic method with an autoanalizer; triglycerides with an enzymatic method by an autoanalizer; an extraction of total fat was done and they were measured by gravimetric, after being dried under nitrogen stream after that it was metilated and the different fatty acids were separated and measured (8-10 C, saturated and unsaturated) by gas chromatography in column ω-wax silica and masses detection. The lipid profile of a sample of industrial food was analyzed.Results. The industrial food is very rich in palmitic acid (16:0) (20.9%), estearic acid(18:0) (6.9%), oleic acid (18:1n-9) (29,7%) and linoleic acid(18:2n-6) (35.1%), being its content in fatty acids of the n3 family, particulary linolenic acid (18:3n-3) (1,0 %).The lipids profile is showed in the table (media ± SD):
Marketed Home Marketed Home
Total fat (g/yolk)
5.3(1.1) 4.5(1.4) 18:3n-6 0.1(0.0) 0.1(0.0)
TG (g/yolk) 2.8(0.7) 2.4(1.0) 18:3n-3** 0.5(0.2) 0.3(0.1)Chol (mg/yolk) 204.2(42.6) 183.8(76.2) 20:1n-9 0.2(0.1) 0.2(0.0)Fatty acids (%weigth//weigth)
20:2n-6*** 0.2(0.1) 0.1(0.0)
14:0 0.4(0.1) 0.4(0.1) 20:3n-6 0.1(0.1) 0.2(0.1)16:0* 25.5(1.9) 27.6(2.8) 20:4n-6 2.2(0.7) 2.5(0.6)16:1n-7 1.5(0.4) 1.9(0.5) 22:4n-6 0.2(0.1) 0.2(0.1)18:0**** 8.9(0.9) 10.8(2.1) 22:5n-3**** 0.1(0.0) 0.2(0.0)18:1n-9 38.0(2.0) 39.5(2.5) 24:0*** 0.0(0.0) 0.1(0.1)18:2n-6**** 18.4(1.3) 11.5(2.1) 22:6n-3 0.9(0.3) 1.3(0.4)
* p < 0.05; ** p< 0.01; *** p<0.005; **** p<0.001 (Kruskal-Wallis test)
Levels of saturated fatty acids, monoinsaturated, n-3 and n-6 families are shown in the figures:
Conclusions. I) In the studied eggs, cholesterol, triglycerides and total fat content are related rather to the egg size that to a diet being for cholesterol around 200 mg. ii) The eggs from hens fed with a diversificate diet and with no commercial fodder have a higher percentage of phospholipids, of saturated fatty acids and mono unsaturated fatty acids versus those fodder- fed hens iii) The percentage of fatty acid n-6 is higher in the commercial eggs and DHA in the household ones iv) The improved fodder can improve the lipid profile of the egg.
1) Makrides M, Hawkes JS, Neumann MA, Gibson RA. “Nutritional effect of including egg yolk in the weaning diet of breast-fed and formula-fed infants: a randomised controlled trial”. Am J Clin Nutr 2002; 76(6):1084-92.
Szymczyk B, Pisulewski PM. “Effects of dietary conjugated linoleic acid on fatty acid composition and cholesterol content of hen egg yolks”. Br J Nutr 2003; 90(1):93-9.
11. DIETARY THERAPY IN OBESE ADOLESCENT. INVEST NUTR ALIM PEDIATR (Rev on-line) 2004; 2. #13. http:// www.seinap.org Lama More R,* Morais Lopez A* Codoceo Alquinta R***Pediatric Nutrition,** Bioquimical DepartmentObesity in adolescent is the most predictive of adult obesity. It is know about the ill effects of obesity in adult patients it was related for diabetes, hipertensión, lipids and cardyovascular disease. But the most weight-loss efforts are ultimately ineffective. There are a several regulatory peptides which modulate feeding onset and offgo: CCK could be saciety hormone at peripherical level. GRP: gastrin release peptide who is downset in obese.GHRELIN1
have been secreted by gastric mucosa and another places of the gastrointestinal tract. It is upset when positive energy balance and obesity.LEPTIN is relased by adipocyte and relationship with intake and the weight when energy store are changing independly to FBM. We have founded down levels of CCK and GRP, Insuline and leptin increased in a obesity children2.AIM: To know the hormonal pattern in relationship with the effect of treatment.Subjects: Patients between 12 – 18 years old with IW >110% and zIBM > +1,89Methods: 1,- Body composition análisis by : a.- Anthropometry with standarized techniquepercentage fat was calculated with use equation of Siry b.- Bioelectrical impedance análisis: To calculate FFM. Quantum II of RJL system.c.- DEXA. 2.- Resting energy expenditure by Deltratrac calorimeter.3.-

Energy intake was evaluated from 24horas-recall and food frecuency methods. Grouping in three: A.- Intake on several times along day. B.- Increased intake on table C.- A+B. 4.- CCK, GRP, Ghr, leptine basal level and at each 10 %weight-loss (RIA). 5.- Dietary treatment: Energy Intake = GER or Energy Intake < GER Weight-loss: 800 – 1000 gr/Week: Protein : 18 – 20%, Fat: 30%, CH: 50 – 52 %. Weekly monitorization of weight and intake 6.- Physical treatment.Statistical análisis: McIntosh JMP and PC: SPSS10Results: 1.- Descriptive analysis.2.-Analysis of statistical differences will be determine in hormone levels over obesity degree, FBM, energy intake and diferent intake mode in repeated measures (t-student, Wilcoxon)3.- Anova will be performed at each evolutive time to assess hormone levels and FBM, FFM, y GER4.- Interaction between Leptina, Ghrelina e insulina and weight-loss at each time will be performer5.- Anova was performed separately for each hormones to assess diferences between zIBM, GER, FBM and intake1.- Murray CDy cols Ghrelin for the gastroenterologist Gastroenterology 2003; 125: 14922.- R Lama, R Codoceo y Cols Leptin in obese children 30th Annual ESPGHAN Meeting, Thesaloniki 1997 12. CHRONOLOGY OF FOOD INTRODUCTION DURING FIRST YEAR OF LIFE IN SPANISH INFANTS. INVEST NUTR ALIM PEDIATR (REV ON-LINE) 2004; 2. #14. HTTP:// WWW.SEINAP.ORG Santamaria-Orleans A1, Miranda-León MT2, Campoy-Folgoso C3
1 Training Dpt, Laboratorios Ordesa, Barcelona, 2 Biostatistics and 3Pediatrics Dpts, Medicine Faculty, University of Granada.Introduction of complementary feeding shows important differences depending on several factors, such as geographical area, training of health professionals responsible of baby follow-up or even socio-economic level of the family. The aim of the present study is to know present characteristics of food diversification in Spanish infants, studying breastfeeding duration, age of introduction of some of the more representatives elements of complementary feeding and influence of the differents geographical and cultural areas on food introduction during the first year of life. Methods: 927 retrospective surveys to mothers of Spanish children (aged between 1-4 years) were carried out, asking about: 1)Socio-demographic data, 2) Information about breastfeeding and infant formula introduction, 3)Information about age of introduction of several foods in infants diet. Statistical Analysis: Normality test (Shapiro-Wilk), Chi2, Wilconson test and Spearman Rho A significance level of 95% was considered. Results: Mean duration of exclusive breastfeeding in Spanish infants is 2,5±2,1 months and mean duration of total breastfeeding 3,8±4,0 months. 27,9% of infants start consumption of infant formula since their birth and only 1,7% maintain exclusive breastfeeding at six months of life. Mean age of complementary feeding introduction is 4,4±1,3 months.Cereals are the first type of food introduced in Spanish infants diet, followed by fruits or cereals and fruits simultaneously. Mean age of gluten free cereals introduction is 4,8±1,4 months and gluten containing cereals are introduced at 7,5±1,8 months. In the case of fruits, orange is the first one which is placed on regular diet of infants (5,2±2,0 months), followed by apple, pear and banana.With reference to animal origen food, chicken presents the earlier age on introduction (6,9±2,2), folloed by beef (7,7±2,5 months) and yogurt (8,5±2,8 months). Mean age of cow milk introduction is Spanish infants is 14,6±4,4 months. 65% of the sample introduced growth (“junior”) milks in theri feeding before consuming cow milk. Statistically significant differences have been found between the different Spanish geograpgical areas in age in complementary feeding start and in age on gluten and cow milk introduction. Conclusions: 1) A low percentage of Spanish infants foloow WHO recommendations about exclusive breastfeeding duration, 2) Complementary feeding introduction take place ina precocious way in relationship to international recommendations, 3) Age of introduction of the different food studied follow, ina general way, recommendations stablished by health authorities, 4) It is necessary to insist to infants care responsibles about the importance of delaying gluten and cow milk introduction in their diet. 13. REGULATION OF FOOD INTAKE; ROLE OF THE HYPOTHALAMUS. INVEST NUTR ALIM PEDIATR (REV ON-LINE) 2004; 2. #15. HTTP:// WWW.SEINAP.ORG Emilio Geijo Barrientos. Alicante
The hypothalamus is one of the main areas of the Central Nervous System (CNS) implicated in regulation of food intake. Hypothalamus acts as a homeostatic control center of many systems critical for survival, such as temperature, reproduction, biological cycles, hormonal balance and energy balance. In the hypothalamus there are a large number of neurotransmitters and peptidic neuromodulators, many of them discovered for the first time in this part of the brain. The hypothalamic area including the arcuate nucleus– medial eminence has a very permeable blood-brain barrier, which makes possible that many substances carried by the blood and that normally do not reach the brain are able to act on this area; this will allow to hypothalamic neurons, in particular those of the arcuate nucleus, to act as sensors of the metabolic state of the organism, this state being measured by blood parameters as glucose, leptin, ghrelin or insulin. Also, there are neurons in the medial and lateral hypothalamus that, acting in coordination with brain stem nuclei, control the gastrointestinal system and other brain areas in order to modify the food intake. In the last years it has been made a great effort to identify those neurotransmitters or neuromodulators implicated in food intake and there have been proposed many candidates to play a critical role in food intake. The key experiment in all these studies is the injection of a particular substance in the hypothalamus or in close brain areas and the observation of eventual short term changes in food intake produced by that substance; some peptides may modify the genomic expression and for that reason they may have long term effects on energy balance. A proper signalling on the hypothalamus by leptin, a peripheral factor depending on the state of the fat deposits of the organism, is critical for the normal control of food intake and corporal weight. leptin signals the nutritional state of the organism to key structures of the hypothalamus and, at the present is considered as a very important signal in the control of energy balance. The administration of leptin, directly on the SNC or to the periphery, produces a decrease in food intake and corporal weight; on the other side, defects in the action of leptin produced either by mutations of the leptin gene or of the leptin receptor gene are associated to massive obesity in man and rodent. The actions of leptin on the hypothalamus are mediated by a large number of neurons that produce orexin or other peptides active on food intake; these neurons are part of the axis arcuate nucleus – paraventricular nucleus – lateral/perifornical hypothalamus. The action of leptin on these neurons is mediated by several intracellular pathways, such as the phosphatidyl inositol kinase – phosphodiesterase 3B – cAMP. A better knowledge of the hypothalamic neuronal circuits and of the actions of substances such as leptin on them is critical, not only to improve our understanding of the role of the hypothalamus on energy balance, but also to the future development of useful drugs to the treatment of food intake disorders in man. 14. BEHAVIOUR, EATING PATTERNS AND OBESITY. INVEST NUTR ALIM PEDIATR (Rev on-line) 2004; 2. #16. http:// www.seinap.org Luis A MorenoE.U. Ciencias de la Salud. Universidad de Zaragoza (Spain)
The prevalence of childhood overweight and obesity has increased in the majority of the countries in the last decades. Epidemiological studies of diet and obesity have focused on single nutrients, most often dietary fat. Intake is usually expressed as a function of energy intake (the percentage of energy from fat). With this approach, many studies did not show that dietary fat is associated with adiposity, independently of total energy intake. Although the relation between dietary fat and obesity remains a subject of continued debate, it is clear that the fat in the diet comes from a variety of foods.
In a recent Spanish survey, the main determinants of obesity in children and adolescents were birth weight lower than 3500 g, absence of breastfeeding, elevated dietary fat intake (>38% of energy), high consumption of industrial pastries and soft drinks, low consumption of fruits and vegetables, and sedentary activities. Only 17.5% of the Spanish children and adolescents consumed more than 2 portions/day of vegetables and 13.29% more than 3 portions/day of fruits.
For the analysis of eating patterns, we can consider a variety of aspects that can include the pattern of meals intake and the frequency of meal intake, snacking habits, beverage consumption, portion sizes, the frequency of restaurant food consumption and the dietary quality. To describe eating patterns in overweight and obese children and adolescents is relevant not only in terms of causality of obesity, but also in terms of the knowledge and understanding of the eating behaviour in the childhood obese individuals. The implications of eating patterns and food consumption in the intake of different nutrients and phytochemicals is also considered.
It seems unlikely that changes in energy intakes, through increased consumption of fast foods, snacks, and soft drinks, have been solely responsible for the increase in body weights in children. Research has shown that low physical activity and high television viewing are also associated with

overweight. The additive effects of these two small changes from traditional behaviour can theoretically lead to large effects on body weight and composition.
The potential modification of eating patterns with the aim of obesity treatment and prevention is a very complex issue, that include attitudes, knowledge and motivation, that can lead to a behavioural change that must be maintained in time. Concerted public health efforts are needed to achieve the healthy objectives for obesity and nutrition and to fight the childhood obesity epidemic. 15. OREXIGÉNICS/ANOREXIGÉNICS DRUGS. INVEST NUTR ALIM PEDIATR (Rev on-line) 2004; 2. #17. http:// www.seinap.org J.F.Horga, Alicante The pharmacology of appetite disorders is undergoing strong changes. The use of drugs with no proved efficacy or unacceptable risk / benefit relationship has been reduced (diuretics, laxatives, hormonal products, catecolaminergic central ways stimulants) and new drugs have been introduced or recovered. For years, orexigénics/anorexigénics drugs that modulate activity of serotonergic nervous system have been assayed and employed. Drugs that induce serotonin release from serotonergic terminals to synaptic cleft (fenfluramine, dexfenfluramine) or inhibit presynaptic reuptake (fluoxetine or sibutramine, that lack pediatric clinical trials) show an anorexigénic effect clinically appreciable, whereas 5-HT-2 receptors antagonists (like ciproheptadine or pizotifen) can act as appetite stimulants. Some of these (fenfluramine group) were withdrawn from the market because of their cardiovascular risk. Subsequently the pharmaceutical industry has introduced drugs that decrease fat absorption by inhibiting pancreatic lipase and preventing the breakdown of dietary fat (orlistat). With the exception of ciproheptadine and pizotifen, none of medicaments listed before is authorized for children administration, and only ciproheptadine has been assayed in children in controlled clinical trials. The discovery of new ways involved in regulation of appetite and satiety is concentrated on study of peripheral and central mechanisms that control neurotransmission in hypothalamic arcuate-paraventricular nuclear complex. In this nuclear system, neuropeptide Y is the main mechanism that induces food intake, and his modifications affect appetite and satiety. Among peripheral mechanisms that regulate synthesis, release and / or effects of neuropeptide Y, and can be drug-controlled, four ways could become defined therapeutic targets. The first is related to inhibition by 5-HT2 serotonergic receptors stimulation of neuropeptide Y effect on paraventricular nucleus. The second is related to leptin, a protein synthesized in fat cells, released to circulation and stimulated by insulin, that has the more critical role as a peripheral sensor of body fat status, and act as a satiety factor reducing synthesis and release on neuropeptide Y; the administration of leptin to ob/ob mutants obese mice reduce food intake and body weight. Third way is related to GHrelin, a peptide released by stomach fundic cells; it can antagonize leptin action through the hypothalamic activation of synthesis and release of neuropeptide Y. GHrelin showed a clear orexigénic effect in rats, and abolish leptin effect in rat hypothalamus. The last way is related to the fragment 3-36 of peptide YY (PYY3-36); this peptide is released from the gut in proportion to the calories ingested, and act inhibiting intestinal motility and neuropeptide Y secretion. Acute PYY3-36 infusion into subjects obese and of normal weight decrease caloric intake during a buffet lunch by 30%. 16. 13C AMINOPYRINE TEST IN LIVER DISEASES IN CHILDHOOD. INVEST NUTR ALIM PEDIATR (REV ON-LINE) 2004; 2. #18. HTTP:// WWW.SEINAP.ORG Tormo R**,*, Segurola H**, Lorite R*, Infante D*, San Nicolás G**Unidad de Gastroenterología Infantil y Nutrición, Hospital Vall d’ Hebron, Barcelona** Unidad de Gatroenterologia Infantil y Nutrición, Via Augusta, BarcelonaThe hepatic mixed function oxidase enzyme system metabolizes a variety of chemotherapeutic agents as well as other benign and noxious compounds ingested from the environment. This enzyme system has the ability to carry out N- and 0- demethylation as well as hydroxylation of individual compounds.The amount of 13C exhaled following the administration of 13C Aminopyrine provides an estimation of the rate of N- demethylation by hepatic microsomes.Post necrosis cirrhosis and alcoholic cirrhosis induces a decrease rate on N- demethylation of aminopirine. Also the decreases on N-demethylation of Aminopririna ia a good marker for liver malgnancy. Partial hepatectomy causes a decrease approximating the amount of liver removed.On the other side, pretreatment with phenobarbital results in an increased hepatic microsomal enzyme mass and causes a proportionate increase in the rate of 13CO2 production.
This test is more sensitive than other based on hidroxylation of other substrates, or prothrombine or serum albumin and alpha 1. .The breath air 13CO2 dosification, after the administration of 13C Aminopyrine allow us to know also the cumulate dosis and the metabolisation speed per hourThe administration of other isotope 13C Methacetin and measurement of 13C in breath air, gives even more information to evaluate the liver functional status .We present our studies concerning the 13C Aminopyrine test on liver diseases in children.MATERIAL AND METHODS13C Aminopyrine was administered at a dose of 2 mg per Kg weight; the breath air was collected on special bags and processed through an Infra Red Spectroscopy Wagner Analyzer; the air was collected at 0 time and every 10 minutes the first hour and every 20 minutes the second hour. The DOB/minutes area under curve (AUC) was calculated. Three groups were stablished::
Group A: 15 children (age range 6 month – 10 years) with normal liver function that had suffered B hepatitis, heterozigous alfa 1 antitripsin defficiency, Wilson disease on treatament or undiagnosed transaminases slight increase; the habitual liver function tests were normal.- Group B: 5 children (age range 6 month – 10 years) with unbalanced portal hypertension ,cirrhosis
and hepatic insufficiency (hepatits B), extrahepatic biliary atresy, 2 patients on hepatic insuficiency for autoimmune hepatitis.
- Group C: 2 patients (age range 8 years – 12 years) before and after treatment for autoimmune hepatitis,
- 1 patient before and after liver transplantation- 1 patient before and after treatment for linfoproliferative disorders.RESULTS:- Group A: AUC mean: 680.04 ; s: 134.58, n: 15- Group B: AUC mean: 114.4; s: 76.5, n:5; mean prothrombine time: 71,5%- (p<0.05)- Group C: - 2 patients before / after liver transplantation: AUC mean 8/ 631; s: 2.82 / 227 - - 2 patients with liver autoimmune hepatits before / after starting immunosupression: - AUC mean:80.5/617; s: 26.16 / 7.07 CONCLUSSIONS: the 13C aminopyrine breath test is a usefull one to study the liver function, easy to perform, quick, non invasive, non expensive and more accurate than many blood serum tests. 17. USEFULNESS OF THE BREATH HYDROGEN TEST IN LACTOSE INTOLERANCE. INVEST NUTR ALIM PEDIATR (REV ON-LINE) 2004; 2. #19. HTTP:// WWW.SEINAP.ORG J.Galiano; M. Juste; E Cortés. ; M. Moya.Servicio de Pediatría. Hospital Universitario. San Juan . AlicantePatients with suspected lactose intolerance are referred from health centers to our out-patient clinic. To diagnose such condition, most institutions in the province of Alicante use the blood glucose curve after oral intake of lactose. In our institution both tests, breath hydrogen test and lactose tolerance test are usually performed.
Symptoms in the patients included in this study (n:30) are:- Recurrent abdominal pain (18 patients)- Chronic diarrhea (6 patients)- Acute diarrhea after dairy products ingestion (4 patients)- Malnutrition (2 patients)As a control group, a breath hydrogen test after lactose overload intake was performed to patients with no gastrointestinal symptomatology (n:20). Obtained median was 5.0 and standard deviation was 0.9.
Thirty-five per cent of patients (5 patients) with abdominal pain had a pathological breath hydrogen test (BH2 > 20); two of them had pain along the test performance. Among these 5, only 3 patients appeared to have abnormal glucose curve. Five patients out of 6 with chronic diarrhea (85 %) had abnormal either breath hydrogen test and glucose curve after oral lactose overload. Only 1 patient (25 %) among those with acute diarrhea after dairy products uptake had abnormal breath hydrogen test and glucose curve after oral lactose overload. Patients with malnutrition had normal results in both tests. All patients with abnormal breath hydrogen test, improved after total or partial lactose withdrawal from diet.
Currently, most institutions in the province of Alicante use the blood glucose curve after oral intake of lactose, we believe that breath hydrogen test should substitute that test, as it is considered suitable to diagnose this condition. 18. THREE COMPONENTS MODEL IN TOTAL BODY COMPOSITION ANALYSIS BY DXA.. INVEST NUTR ALIM PEDIATR (Rev on-line) 2004; 2. #20. http:// www.seinap.org L del Río*; A. Carrascosa**; D. Yeste**. (*)Cetir Centre Mèdic. (**)Hospital Materno Infantil Valle de Hebron. Barcelona. España.From birth to the end of the puberal period the healthy children show dramatic changes in body composition with significative increase of bone mineral content, fat mass and lean mass.The aim to the present study was assesses the changes in body composition (BC) from childhood to young hood and allow the influence of sex maturation from 2 to 21 years. A group of 1072 white healthy volunteers (302 male and 780 female), from the urban area of Barcelona. Bone mineral content (BMC), Bone mineral density (BMD), fat mass and lean mass were measured by a dual-energy ray-x absoprtiometry (DXA) device (Prodigy, GE-Lunar). Puberal stage was evaluated by Tanner method. BMC and BMD values progressively increase and mean values were similar in both sexes until to age of 10. BMD mean values were similar in both sex (2-21years) However, total BMC values were higher in girls than in boys between the age 11-16 y (p<0.001). Regional analysis shown higher arms and legs BMC values in boys than girls in 10-16 y. of age (p<0.0001 - p<0.03 respectively) whereas girls showed higher values in BMC pelvis (p< 0.08). Fat mass and lean mass in girls showed same trend in each age group (2-21 y. of age). On the other hand, fat mass in boys showed a significant decrease and simultaneously a significant lean mass increase. Significant differences were noticed for distribution amongst both sexes for ages going from 14 through 19 years. Both soft tissue compartments increased in a similar way in females from pubertal stage. There was an opposed tendency for males, characterized by an increase in lean mass in this life period while the fatty mass decreased.CONCLUSIONSThe body size difference between teenagers and young adults in relationship with sex justified the BMC differences found after the absence of significant DMO differences.Genetic and hormonal factors may be responsible for a different evolutive tendency in fat mass and lean mass between sexes during growth and maturation.The regional differences in BMC, BMD in limbs can be related to the different physical activity pattern followed by male individuals as opposed to the female ones.
19. EXPRESSIONN OF MICA FOLLOWING ACUTE EXPOSURE TO GLIADIN ON THE INTESTINAL MUCOSA OF TREATED CELIAC PATIENTS ON GLUTEN-FREE DIET. INVEST NUTR ALIM PEDIATR (REV ON-LINE) 2004; 2. #21. HTTP:// WWW.SEINAP.ORG Juan Carlos Vitoria, Ainhoa Martín-Pagola, Gustavo Pérez-Nanclares, Lourdes Ortiz-Paranza , J. Ramón Bilbao, Luis Castaño.Departamento of Pediatrics and Research Unit. Hospital de Cruces. BilbaoThe contribution of HLA class II genes to celiac disease (CD) risk has been known for some time. During the last few years, the existence of another CD-predisposing locus in the telomeric region of chromosome 6p has been pointed out.MICA is located in this region and has been proposed as a putative candidate involved in CD development, based on its expression in the gastrointestinal epithelium and its function a stress-induced immune activator. Ingestion of gluten in CD could serve as a stress signal for epithelial cells and could uprregulate MICA expression on their surface. It could thus be possible that MICA is functionally implicated in the activation of the immune response in the gut.In a previous study we investigated whether MICA expression was increasd among non-treated CD patients, compared to patients on gluten free diet (GFD) and non-celiac controls.Quantitative analysis by RT-PCR of intestinal biopsies of treated and untreated celiac patients and non-celiac controls detected production of MICA mRNA, but no differences were seen among the three groups. Nevertheless, when IFNG mRNA was analyzed in the same samples, there was an increased expression of this cytokine among CD patients at diagnosis, comparaded to treated CD patients and controls.
MICA does not seem to play an important role in CD pathogenesis, at least in the final stages of disease development just before diagnosis. It could be that overexpression of MICA takes place at the initial phases of the intestinal lesion, to rapidly return to basal levels.The aim of the present study was to determine whether MICA expression is increased in normalized biopsies of CD patients on GFD for over two years, when they are acutely exposed to gliadin.Patients and MethodsWe studies 7 biopsies from CD patients of GFD and 5 controls. Biopsies were divided in two and incubated in RPMI culture medium with and without 10 mg/ml gliadin, at 37ºC and 5% CO2 for 4 hours. On the same day, blood samples were drawn for genetic testing (MICA and HLA-DQ) and anti-transglutaminase autoantibody determinations. After incubation, MICA mRNA was quantified using RT-PCR with specific primers and compared to GAPDH gene expression.ResultsExpression of MICA was observed among patients and controls, but gliadin incubation induced a large increase among treated CD patients compared to controls.ConclusionsGliadin provokes overexpression of MICA on normalized intestinal mucosa of treated CD patients. This suggests a role during the first stages of autoimmune destruction of the intestinal mucosa, probably preceeding the onset of inflammation. 20. GENETICS ASPECTS OF CYSTIC FIBROSIS. RELATIONSHIPS WITH PHENOTYPE. INVEST NUTR ALIM PEDIATR (REV ON-LINE) 2004; 2. #22. HTTP:// WWW.SEINAP.ORG JA Gómez-Capilla 1 , A Gómez-Llorente1, M Navarro2, C Campoy3
1Departament of Biochemistry and Molecular Biology. School of Medicine. University of Granada. 2Departament of Paediatrics. University Hospital Virgen de la Macarena. Infant Pneumology Service. Sevilla. 3Departament of Paediatrics. School of Medicine. University of Granada.CFTR mutation located in the short arm of 7 chromosome determines the Cystic Fibrosis (CF). There are more than 1000 different mutations which are responsible of the illness, varying on frequency depending on the population studied. The studies done in the CFTR gene in different population, have shown the presence of considerable differences in the frequency of the most common mutations, such as ∆F508, N1303K, G551D or W1282X. The heterogeneity in the clinic expression of the illness, specially regarding the gravity, age at the beginning, and progression, as well as the alteration of pancreatic exocrine, lung, reproduction in males or sweat Cl- concentrations, joined to the high number of CFTR gene mutations found, have increased the interest to find a relationship between the mutation and the clinic expression of the illness. Aim: To analyse the clinical expression of the CF in 55 Andalusian’s children studied retrospectively to establish a relationship between genotype and phenotype to develop early therapeutic methods to act.Methods: The patients were diagnosed of CF in the Laboratory of Molecular Genetics in the Biochemical Department of the Granada’s University. The modified “Applied Biosystem” method was used for the genetics analysis which is able to detect simultaneously 31 mutations using 15 µL of fresh blood. Statistical analysis: Fisher’s test, Chi2 test, and relative risk (RR) calculation. Results: In the population studied, 8 different mutations of the CFTR gene have been found: ∆F508, G542X, R334W, R1162X, 2789+5G→A, R117H, ∆I507 and W1282X. From the 55 patients studied at diagnostic moment, the 69.6% had respiratory symptoms and the 35.89% chronic toss; air flux obstruction was demonstrated in the 30.76%, radiological alterations in the 28.20% and CF typical microbial colonization in the 5.12%. The digestive manifestations were present in the 44.5% of the total of patients studied, in the following order: 45.8% nutritional pathology, 41.65% pancreatic illness, 11.2% intestinal alteration. There were no significant correlations between the respiratory
symptoms and the genetic study. There was a significant correlation between the ∆F508 homocygosis and pancreatic pathology. The RR showed that the homocygotic patients (∆F508) show 4 fold higher risk to develop nutritional pathology with a range between 1.50≤RR<10.66. Homocygosis has also a tendency to develop twice more intestinal pathology with a
range between 1.26≤ RR<5.65, indicating that in some cases this risk could be even >5 times higher than the heterocygotic individuals.Conclusion: ∆F508 homocygosis is related with the possibility to suffer digestive pathology in general, nutritional alterations, intestinal pathology, and specially a high risk of pancreatic pathology. 21. HEPATIC STEATOSIS AND OBESITY. INVEST NUTR ALIM PEDIATR (Rev on-line) 2004; 2. #23. http:// www.seinap.org Peña L, Colino E, Saavedra P, Quintana M, Cazenave E, Ramos JC, Quinteiro S, Domínguez AHospital Universitario Materno-Infantil de Canarias. Las Palmas de Gran CanariaIntroduction: Hepatic steatosis is frequently found in obese children and adolescents but its exact phisiopathology remains unclear. Objectives: To relate hepatic steatosis with cardiovascular risk factors and other biochemical parameters in obese children.Patients & Methods: 104 obese children and adolescents (BMI and skinfolds > P95) aged 4-14 years (mean 10.8 ± 2.50; 52 boys / 48 girls) and 99 control children and adolescents aged 4-14 years (mean 10.8 ± 2.52; 51 boys / 48 girls) (Tanner 1-4) were included in this transversal study. Syndromic and endocrinological origins were ruled out. A detailed anamnesis, a lifestyle questionnaire and a careful clinical exploration (including blood pressure and a dietetic evaluation) were performed; emotional state and exercise level were also checked. Hematimetry, leptin, lipids, hepatocellular function, microalbuminary, insulinresistance (HOMA), insulinsensitivity (basal insulinemia and glycaemia/insulin index), and other parameters were determined. Children in the obese group underwent an oral glucose tolerance test, an abdominal ecography and it was studied the presence of acanhtosis nigricans. For those patients with hepatic steatosis, known causes of chronic hepatopaty were excluded. Statistical analisis was performed by the software package SPSS-PC.Results: The prevalence of hepatic steatosis in obese children was 18.8%, being more frequent in boys than in girls (27.1% vs 10.4%) (p=0.036). The higher the time of evolution, the higher the proportion, reaching significance when time of evolution > 5 years (25% vs 10%) (p=0.03). Only 5 out of 18 (27.7%) children with steatosis showed raised transaminase levels. Obviously, raised levels of GGT, AST and ALT were clearly related to hepatic steatosis (p=0.056, p=0.001, p=0.000, respectively). When comparing obese children with and without steatosis, a clear relationship was found with hyperinsulinemia (p=0.000) and triglycerides (> 150) (p=0.018), as well as with acanthosis nigricans (p=0.006), but not with total cholesterol, C-LDL, C-HDL, glycaemia, leptin, Tanner stage, or exercise. All patients were clinically asymptomaticConclusions: Hepatic steatosis should be ruled out in obese children through imaging methods and it is related to time of evolution, hypertriglyceridemia and hyperinsulinemia. 22. HOMOCYSTEINE AND ATHEROSCLEROSIS. INVEST NUTR ALIM PEDIATR (REV ON-
LINE) 2004; 2. #24. HTTP:// WWW.SEINAP.ORG Ángel Gil Department of Biochemistry and Molecular Biology; University of Granada, Spain Homocysteine is a sulphur-containing amino acid formed during the metabolism of methionine by the remethylation or transsulfuration pathways. In the remethylation cycle, homocysteine is salvaged by the acquisition of a methyl group in a reaction catalysed by methionine synthase, which has vitamin B12
as an essential cofactor. N5-methyltetrahydrofolate (Me-THF) is the methyl donor in this reaction, and N5, N10 Me-THF reductase functions as a catalyst. In the transsulfuration pathway, homocysteine condensates with serine, a reaction catalysed by the vitamin B6-dependent enzyme cystathionine β-synthase, rendering cystathonine and later cysteine.
There are numerous clinical observations linking elevated plasma homocysteine concentrations with vascular disease. The first report relating extensive thrombosis and atherosclerosis was published in 1969 in two children with homocysteinemia and homocystinuria. Subsequent investigations have clearly

demonstrated that hyperhomocysteinemia is an independent risk factor for atherosclerosis and atherothrombosis in coronary, cerebral, and peripheral vasculature. Although severe hyperhomocysteinemia is rare, mild plasma levels of homocysteine occur in approximately 5-7% of the general population. In these subjects, typically asymptomatic until the third to fourth decade of life, premature coronary artery disease develops, as well as, recurrent arterial and venous thrombosis. Protein-bound homocyst(e)ine accounts for 70-80% of the total plasma pool. Normal concentrations range 5-15 µmol/l and moderate concentration 15-30 µmol/l.. Hyperhomocyst(e)inemia is considered to be present if the homocysteine concentration after 4-8 h of 100 mg/ kg body weight methionine challenge is more that 2SD above the mean., although the prognostic value of this test is less valuable in persons with the thermolabile variant of N5, N10 Me-THF reductase. Elevations in plasma homocysteine are typically caused by genetic defects in the enzymes involved in the metabolism of this amino acid or by nutritional deficiencies in vitamin cofactors. Cystathionine β-synthase deficiency is the most common genetic cause of severe hyperhomocysteinemia (congenital homocystinuria). A homologous deficiency of N5, N10 Me-THF reductase may also lead to severe hyperhomocysteinemia. The thermolabile variant of this last enzyme is caused by a point mutation (C677T) in the coding region for THF binding site and correlates with elevated plasma levels of homocysteine. Homozygous persons for this mutation have an exaggerated hyperhomocysteinemic response to the depletion of folic acid and increased risk for cardiovascular disease. Nutritional deficiencies of folate, vitamin B12 and vitamin B6 may also promote hyperhomocysteinemia. In fact, inadequate plasma concentrations of one or more B vitamins are contributing factors in approximately two thirds of hyperhomocysteinemia. High levels of this amino acid can also be found in chronic renal failure, hypothyroidism, and cancer.
Experimental evidence suggests that the atherogenic propensity associated with hyperhomocisteinemia results from endothelial dysfunction and injury followed by platelet activation and thrombus formation. Homocysteine is rapidly auto-oxidised forming homocystine, mixed disulfides and homocysteine thiolactone; powerful reactive oxygen species are formed in this process, which in turn cause vascular injury and toxicity, mainly due to increased LDL oxidation and alteration of the antithrombotic phenotype, enhanced production of NO, increased expression of cyclins D1 and A, and activation of the pro-inflammatory transcription factor NF-κB. 23. OBESITY AS A GLOBAL EPIDEMIE IN CHILDREN AND ADOLESCENTS. PREVENTION STRATEGIES. INVEST NUTR ALIM PEDIATR (Rev on-line) 2004; 2. #25. http:// www.seinap.org R. Tojo, R. LeisUnidad de Investigación en Nutrición y Desarrollo Humano de Galicia. Cátedra Novartis Medical Nutrition-Universidad de Santiago de Compostela de Nutrición Clínica Pediátrica. Departamento de Pediatría. Hospital Clínico Universitario de Santiago. USC. España.The International Obesity Task Force (IOTF) report to the World Health Organisation (WHO) estimates that around a 10% of children and adolescents between 5-17 years old have overweight, and among them a 2-3% are obese, which means some 155 millions with overweight and approximately 40 millions with obesity. Thus, obesity in children and adolescents represents an important public health problem, where paediatricians must be involved with determination, but also with training and means, not only technical but also professional, making a task force with dieticians, psychologists, specialists in physical activity, which allows to proceed both on the child and family as well as on school, society, community, public powers, industry and mass media. The fast progression of childhood obesity prevalence during the last two decades (in Spain it has tripled) shows that genetic factors are not to be the first reason of the change, although studies in twins show the genetic predisposal to gain weight must represent a 60-85% of the obesity variation. The theory of the saving genes establishes that these favoured the survival of the specie at facilitating its ability to use and store energy during the long periods of food shortage and great physical activity, which were typical of our evolution. Now, in an obesogenic environment, characterised by the abundance of food and the laziness to make any physical activity, the expression of obesity is evident. Nowadays, the universal access to information, communication and knowledge technologies (ICTs) is linked to an obesogenic diet and less degree of physical activity in a determining way. These technologies are every time more omnipresent in children’s lives, as well as television, videos, computers, Internet, mobile telephones, which next to transport and journey motorization favour a non-active life. By now, there are no miracle pills or genetic therapy for obesity, so the main objective for paediatricians must be to prevent it. The major justification as professionals and children defenders is that already from

the first decade of life, obesity favours the development of comorbilities, which affect most organs and systems in children and adolescents. The most severe the obesity, greater the risk of dyslipemia, high blood pressure, glucose and insulin metabolism alteration, including type 2 diabetes, which favour the development of metabolic syndrome, atherogenesis, chronic inflammation, endothelial dysfunction and cardiovascular risk. But sleep apnea and asthma, non alcoholic fatty liver disease, muscle-skeleton alterations, the pseudotumor cerebri, renal alterations and especially psychosocial disorders are also essential. Moreover, as it is a chronic disease, the risk for the obese child to be an obese adult is real and, consequently, morbidity and premature mortality risks are also existent.The prevention, following the WHO recommendations, must involve in a simultaneous complementary coordinated action all those international, national, regional and local legislative and executive organisms, food industry, ICTs, non official organisations, NGO’s, school, family and child. Besides, prevention strategies must be progressive: universal prevention, aimed to all the paediatric population, selective prevention, aimed to higher than average risk groups and target prevention, aimed to high risk groups, those who already show overweight, but are not obese yet.Risk factors may already be present in prenatal stages, so health, nutritional state and diet in pregnant woman are a priority. The weight at birth, the weight one year later, the evolution of the weight speed and the BMI in the first years are some factors to be taken into account as well as breast milk or formula feeding and the beginning and kind of complementary food. The socioeconomic and educational level, especially the mother’s, and the obesity family history deserve priority attention.General objectives:
• To prevent excessive weight and BMI gain: Diminishing energy intake and the intake of food rich in saturated fat and trans and rich in
carbohydrates with a high glycemic index and loads. Diminishing the size of the portions, fast food, snacks and soft drinks, eating in front of the TV, the exposure to manufactured food and drink advertising and eating outside home.
Increasing fruit, vegetable, whole grain, fibre, mono and polyunsaturated fats and bioactive components intake. Improving the quality of school menus and increasing the frequency of family meals.
Increasing the energy expense, increasing physical activity, structured or not (games, physical training, school sports, home activities, extracurricular and weekend activities).
Diminishing sedentary activity. Walking, climbing stairs instead of getting the lift or escalators, using a bicycle instead of the school bus or the family car. Diminishing the time spent with ICTs, especially television. Favouring the development of new areas to practice sports and games, safe school routes, which allow the promotion of active ways of life during leisure and spare time, both for the child and his/her family.
Recent articles reveal the controversies that still exist about the reasons for the paediatric obesity epidemie. But in any way, the physical inactivity and the low quality diet obviously contribute, especially the carbohydrates high intake (fast foods) with a high glycemic loads and index due and bad fats, to the alterations they produce in the glucose and insulin metabolism and in hunger and satiety control mechanisms.The preventive strategies of paediatric obesity need a conductual support and be made inside the family and school environments.It must be present that these paediatric strategies may have little success, because there exist important powerful barriers which are against the change from an obesogenic diet to a healthy one and from inactivity to activity. The food industry, TV advertising, ICTs abuse, the parents’ limited time dedicated to children, the school little implication in children’s healthy patterns and the more inclined habitat to a sedentary lifestyle than to activity are some of the reasons. It is the paediatricians right and duty to leader and be active in the promotion of such a change.BibliographyBowman SA, Gortmaker SL, Ebbeling CB, Pereira MA, Ludwig DS. Effects of fast-food consumption on energy intake and diet quality among children in a National Household Survery. Pediatrics 2004; 113: 112-18.Lobstein T, Bauer L, Uauy R. For the IASO International Obesity Task Force. Obesity in children and young people: a crisis in public health. Obes Rew 2004; 5 (suppl. 1): 4-85.Slyper AH. The pediatric obesity epidemie: Causes and controversies. J Clin Endocrinol Metab 2004; 89 (6): 2540-7.Stettler JR. The global epidemie of childhood obesity: is there a role for the paediatrician?. Obes Rew 2004; 5 (suppl. 1): 1-3.
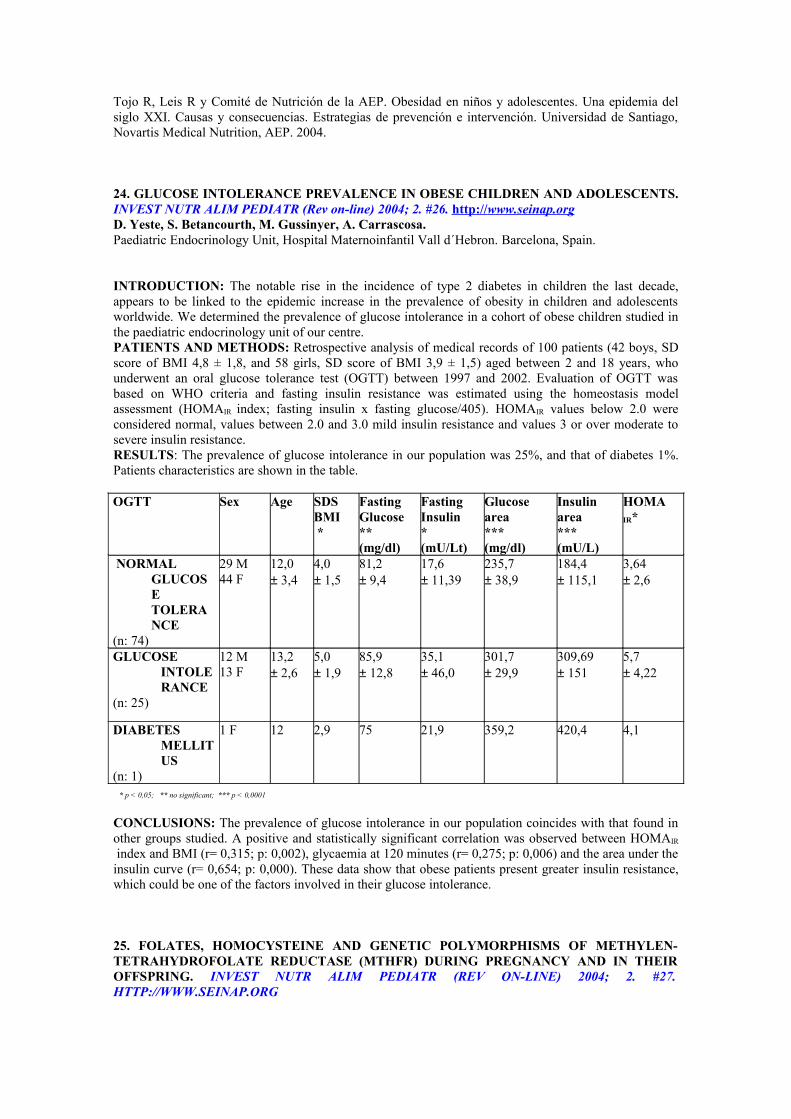
Tojo R, Leis R y Comité de Nutrición de la AEP. Obesidad en niños y adolescentes. Una epidemia del siglo XXI. Causas y consecuencias. Estrategias de prevención e intervención. Universidad de Santiago, Novartis Medical Nutrition, AEP. 2004. 24. GLUCOSE INTOLERANCE PREVALENCE IN OBESE CHILDREN AND ADOLESCENTS. INVEST NUTR ALIM PEDIATR (Rev on-line) 2004; 2. #26. http:// www.seinap.org D. Yeste, S. Betancourth, M. Gussinyer, A. Carrascosa.Paediatric Endocrinology Unit, Hospital Maternoinfantil Vall d´Hebron. Barcelona, Spain.
INTRODUCTION: The notable rise in the incidence of type 2 diabetes in children the last decade, appears to be linked to the epidemic increase in the prevalence of obesity in children and adolescents worldwide. We determined the prevalence of glucose intolerance in a cohort of obese children studied in the paediatric endocrinology unit of our centre.PATIENTS AND METHODS: Retrospective analysis of medical records of 100 patients (42 boys, SD score of BMI 4,8 ± 1,8, and 58 girls, SD score of BMI 3,9 ± 1,5) aged between 2 and 18 years, who underwent an oral glucose tolerance test (OGTT) between 1997 and 2002. Evaluation of OGTT was based on WHO criteria and fasting insulin resistance was estimated using the homeostasis model assessment (HOMAIR index; fasting insulin x fasting glucose/405). HOMAIR values below 2.0 were considered normal, values between 2.0 and 3.0 mild insulin resistance and values 3 or over moderate to severe insulin resistance.RESULTS: The prevalence of glucose intolerance in our population was 25%, and that of diabetes 1%. Patients characteristics are shown in the table.SEXO
a* p < 0,05; ** no significant; *** p < 0,0001
EDADCONCLUSIONS: The prevalence of glucose intolerance in our population coincides with that found in other groups studied. A positive and statistically significant correlation was observed between HOMAIR
index and BMI (r= 0,315; p: 0,002), glycaemia at 120 minutes (r= 0,275; p: 0,006) and the area under the insulin curve (r= 0,654; p: 0,000). These data show that obese patients present greater insulin resistance, which could be one of the factors involved in their glucose intolerance. 25. FOLATES, HOMOCYSTEINE AND GENETIC POLYMORPHISMS OF METHYLEN-TETRAHYDROFOLATE REDUCTASE (MTHFR) DURING PREGNANCY AND IN THEIR OFFSPRING. INVEST NUTR ALIM PEDIATR (REV ON-LINE) 2004; 2. #27. HTTP://WWW.SEINAP.ORG
OGTT Sex Age SDS BMI *
Fasting Glucose**(mg/dl)
Fasting Insulin*(mU/Lt)
Glucose area***(mg/dl)
Insulin area ***(mU/L)
HOMA IR*
NORMAL GLUCOSE TOLERANCE
(n: 74)
29 M44 F
12,0± 3,4
4,0± 1,5
81,2± 9,4
17,6± 11,39
235,7± 38,9
184,4± 115,1
3,64± 2,6
GLUCOSE INTOLERANCE
(n: 25)
12 M13 F
13,2± 2,6
5,0± 1,9
85,9± 12,8
35,1± 46,0
301,7± 29,9
309,69± 151
5,7± 4,22
DIABETES MELLITUS
(n: 1)
1 F 12 2,9 75 21,9 359,2 420,4 4,1
JA Molina-Font1, Dolz V1, Linde J2, Molloy A3, Scott J3, Pardillo S4, Decsi T5, Koletzko B6, Gil A2, Campoy C1
1Dept. of Paediatrics. School of Medicine. University of Granada. Spain. 2Dep. of Biochemistry and Molecular Biology. School of Pharmacy. University of Granada. Spain. 3Dept. of Biochemistry and Molecular Biology. Division of Nutrition and Folic Acid. Trinity College. Dublin (Ireland). 4Dept. of Obstetric and Gynecology. Granada´s University Hospital San Cecilio. 5Dept. of Paediatrics, University of Pécs. Hungary. 6Dr. v. Haunersches Kinderspital, LMU München. Germany. High homocysteine plasma concentrations (tHcys) are considered as a risk cardiovascular factor and are a sensible biomarker about the vitamin B12 and folate nutritional status. The hyperhomocystinemia (HtHcys) has been related to foetal toxicity due to DNA alterations, hypometilation or insufficient synthesis of DNA, or due to structural damage in the genes implied in the DNA synthesis. Folic acid (FAc) deficiency could change the long chain polyunsaturated fatty acids metabolism (LC-PUFAs). The enzyme metilen-tetrahydrofolate reductase (MTHFR) improve the conversion of 5,10-Metilentetrahydrofolate (5,10-MTHF) to 5-MTHF and has a direct influence on the re-metilation of Hcys to Methionine. The most common mutation of the MTHFR is the substitution of Cytosine instead of Timine in the 677 base. The 677TT homocygosis determines a low MTHFR activity related to neural tube defects and HtHcys. A total of 155 Spanish healthy pregnant women participants in the NUHEAL study; aged between 18 and 40 years, were recruited at the 20±1 wks of gestation. Following a double blind & random design, were subdivided into 4 groups, depending on the supplement received until delivery (DHA: 0.5 g/day; 5-MTHF: 0.4 mg/day; both or placebo). In this study the effects of the different supplements received by the mothers during pregnancy on the FAc and tHcys plasma concentrations, and on the genetic polymorphism of the MTHFR are studied. Biochemical analysis: MTHFR Genetic polymorphisms: PCR; tHcys in µmol/L: HPLC; FAcs (serum) in nmol/L and Face (erythrocytes) in ng/ml: O'Broin and Kelleher method (1992). Plasma LC-PUFAs were obtained by gas chromatography. Statistical analysis: ANOVA, General Lineal Model for repeated measures and correlation analysis. *: p<0.005. Results: Mother’s serum tHcys values and in their newborns were <15 µmol/L. At the end of pregnancy the tHcys was higher in the mothers which received DHA exclusively and in the placebo group in front of the groups which received 5-MTHF (DHA: 6.39±0.32; 5-MTHF: 5.61±0.28*; Placebo: 6.37±0.33; DHA+5-MTHF: 5.67±0.22*). FAcs levels ware <9 nmol/L in the 39% of the pregnant women at the beginning of the study, in the 60% in the 30 th weeks and in the 56% at delivery. AcFe concentrations were < 225 ng/ml in the 45.4% at 20 weeks, in the 72% at 30th weeks and in the 70% at delivery. The 12.6% of the neonates showed deficiency of Folic acid. Although the MTHFR 677C T polymorphism is considered the most common in the population, was only present in the 30.1% of the mothers and in the 41.7% of the neonates. The 19.6% of the mothers and the 11.9% of the newborn infants had MTHFR homocygosis (677TT). The MTHFR 677CC polymorphism was the most frequent in our cohort (41.3% mothers/ 46.4% neonates). Different significant correlations between FAcs, Face and tHcys and LC-PUFAs were established, as well as between these parameters between placenta one side and the other. Conclusions: Mother’s FAc nutricional status decreases during pregnancy, and it is correlated with the FAc nutritional status in their offspring. 677TT genotype determines a higher risk of FAc deficiency in the mother and in the neonate. A placental protector mechanism is suggested to avoid the HtHcys in the neonate despite the increasing of the concentrations in the mother.This work is a part of the 5th EU Framework Program (Research grant Nutrition and Healthy Lifestyle [NUHEAL], grant no. CLK1-CT-1999-00888). 26. LEPTIN LEVELS DURING THE FIRST YEAR OF LIFE IN LOW AND VERY LOW BIRTH WEIGHT INFANTS. INVEST NUTR ALIM PEDIATR (Rev on-line) 2004; 2. #28. http:// www.seinap.org N M Díaz-Gómez*, E Doménech**, F Barroso**, C Cortabarria**, S Castells*, A Jiménez#.* E.U.Enfermería y Fisioterapia. ** Facultad de Medicina. Universidad de La Laguna. # Unidad de Investigación del Hospital Universitario de Canarias. Tenerife.Low birth weight may increase the later risk of metabolic syndrome which includes obesity and diabetes, but the mechanisms involved are uncertain. Programming of both leptin and insulin-growth-factor-1 (IGF-1) concentration may be one mechanism by which early nutrition influences later obesity. Little is known concerning the inter-relation between leptin and IGF-1 and their role in the control of body composition in low birth weight infants.Objective: To study the changes in the pattern of leptin, IGF-1 and their binding-protein: IGFBP-1 and IGFBP-3, in the first year of life, in preterm infants and their relationship with body composition.
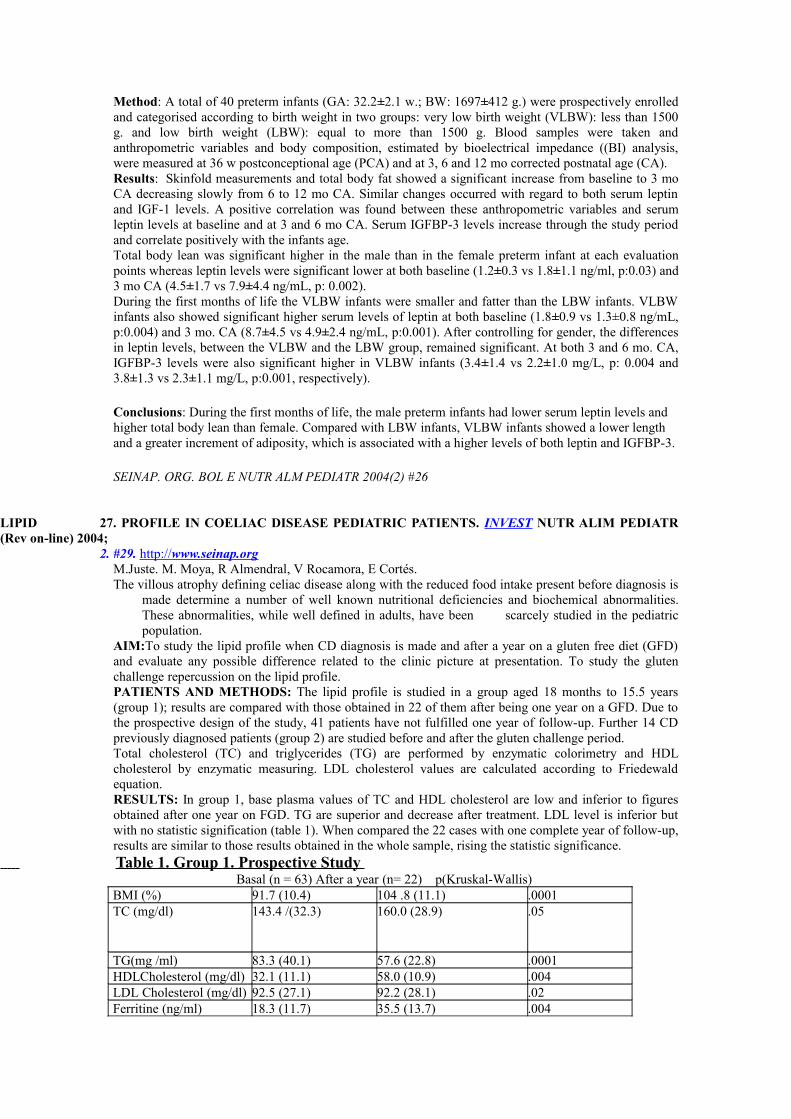
Method: A total of 40 preterm infants (GA: 32.2±2.1 w.; BW: 1697±412 g.) were prospectively enrolled and categorised according to birth weight in two groups: very low birth weight (VLBW): less than 1500 g. and low birth weight (LBW): equal to more than 1500 g. Blood samples were taken and anthropometric variables and body composition, estimated by bioelectrical impedance ((BI) analysis, were measured at 36 w postconceptional age (PCA) and at 3, 6 and 12 mo corrected postnatal age (CA).Results: Skinfold measurements and total body fat showed a significant increase from baseline to 3 mo CA decreasing slowly from 6 to 12 mo CA. Similar changes occurred with regard to both serum leptin and IGF-1 levels. A positive correlation was found between these anthropometric variables and serum leptin levels at baseline and at 3 and 6 mo CA. Serum IGFBP-3 levels increase through the study period and correlate positively with the infants age. Total body lean was significant higher in the male than in the female preterm infant at each evaluation points whereas leptin levels were significant lower at both baseline (1.2±0.3 vs 1.8±1.1 ng/ml, p:0.03) and 3 mo CA (4.5±1.7 vs 7.9±4.4 ng/mL, p: 0.002). During the first months of life the VLBW infants were smaller and fatter than the LBW infants. VLBW infants also showed significant higher serum levels of leptin at both baseline (1.8±0.9 vs 1.3±0.8 ng/mL, p:0.004) and 3 mo. CA (8.7±4.5 vs 4.9±2.4 ng/mL, p:0.001). After controlling for gender, the differences in leptin levels, between the VLBW and the LBW group, remained significant. At both 3 and 6 mo. CA, IGFBP-3 levels were also significant higher in VLBW infants (3.4±1.4 vs 2.2±1.0 mg/L, p: 0.004 and 3.8±1.3 vs 2.3±1.1 mg/L, p:0.001, respectively).
Conclusions: During the first months of life, the male preterm infants had lower serum leptin levels and higher total body lean than female. Compared with LBW infants, VLBW infants showed a lower length and a greater increment of adiposity, which is associated with a higher levels of both leptin and IGFBP-3.
SEINAP. ORG. BOL E NUTR ALM PEDIATR 2004(2) #26
LIPID 27. PROFILE IN COELIAC DISEASE PEDIATRIC PATIENTS. INVEST NUTR ALIM PEDIATR (Rev on-line) 2004; 2. #29. http:// www.seinap.org
M.Juste. M. Moya, R Almendral, V Rocamora, E Cortés.The villous atrophy defining celiac disease along with the reduced food intake present before diagnosis is
made determine a number of well known nutritional deficiencies and biochemical abnormalities. These abnormalities, while well defined in adults, have been scarcely studied in the pediatric population.
AIM:To study the lipid profile when CD diagnosis is made and after a year on a gluten free diet (GFD) and evaluate any possible difference related to the clinic picture at presentation. To study the gluten challenge repercussion on the lipid profile.PATIENTS AND METHODS: The lipid profile is studied in a group aged 18 months to 15.5 years (group 1); results are compared with those obtained in 22 of them after being one year on a GFD. Due to the prospective design of the study, 41 patients have not fulfilled one year of follow-up. Further 14 CD previously diagnosed patients (group 2) are studied before and after the gluten challenge period.Total cholesterol (TC) and triglycerides (TG) are performed by enzymatic colorimetry and HDL cholesterol by enzymatic measuring. LDL cholesterol values are calculated according to Friedewald equation.RESULTS: In group 1, base plasma values of TC and HDL cholesterol are low and inferior to figures obtained after one year on FGD. TG are superior and decrease after treatment. LDL level is inferior but with no statistic signification (table 1). When compared the 22 cases with one complete year of follow-up, results are similar to those results obtained in the whole sample, rising the statistic significance.
Table 1. Group 1. Prospective Study Basal (n = 63) After a year (n= 22) p(Kruskal-Wallis)BMI (%) 91.7 (10.4) 104 .8 (11.1) .0001TC (mg/dl) 143.4 /(32.3) 160.0 (28.9) .05
TG(mg /ml) 83.3 (40.1) 57.6 (22.8) .0001HDLCholesterol (mg/dl) 32.1 (11.1) 58.0 (10.9) .004LDL Cholesterol (mg/dl) 92.5 (27.1) 92.2 (28.1) .02Ferritine (ng/ml) 18.3 (11.7) 35.5 (13.7) .004
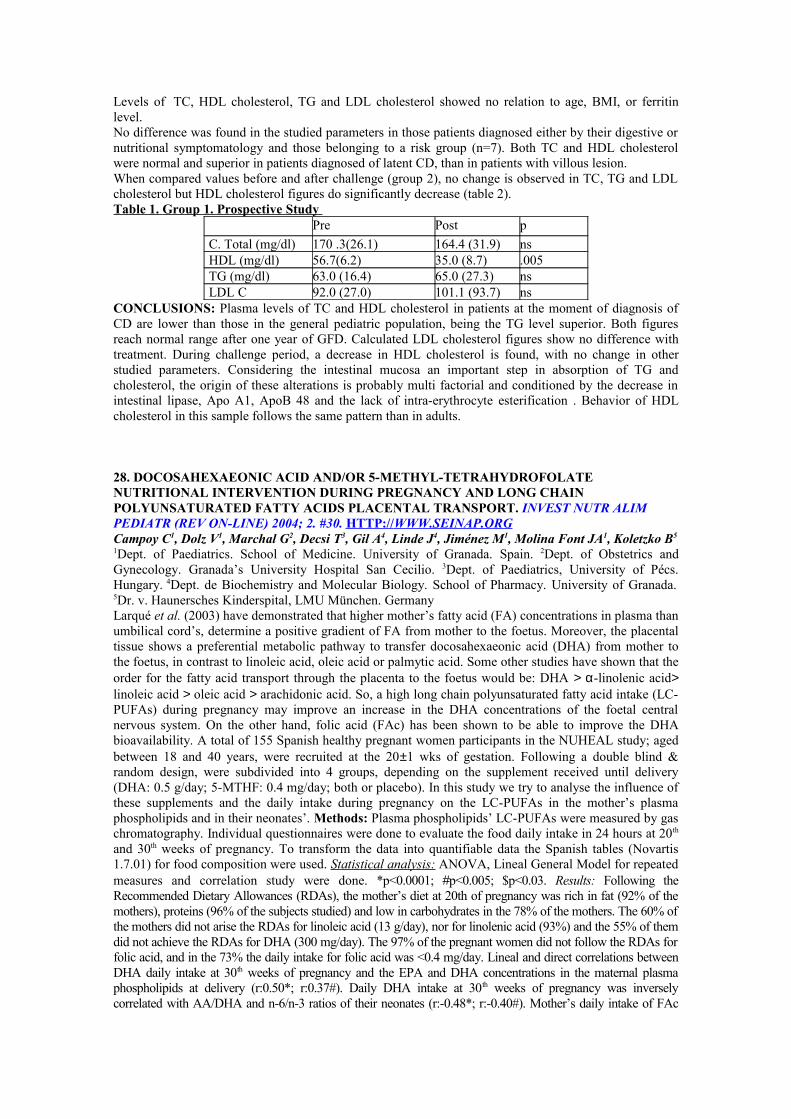
Levels of TC, HDL cholesterol, TG and LDL cholesterol showed no relation to age, BMI, or ferritin level.No difference was found in the studied parameters in those patients diagnosed either by their digestive or nutritional symptomatology and those belonging to a risk group (n=7). Both TC and HDL cholesterol were normal and superior in patients diagnosed of latent CD, than in patients with villous lesion.When compared values before and after challenge (group 2), no change is observed in TC, TG and LDL cholesterol but HDL cholesterol figures do significantly decrease (table 2).Table 1. Group 1. Prospective Study
Pre Post p
C. Total (mg/dl) 170 .3(26.1) 164.4 (31.9) nsHDL (mg/dl) 56.7(6.2) 35.0 (8.7) .005TG (mg/dl) 63.0 (16.4) 65.0 (27.3) nsLDL C 92.0 (27.0) 101.1 (93.7) ns
CONCLUSIONS: Plasma levels of TC and HDL cholesterol in patients at the moment of diagnosis of CD are lower than those in the general pediatric population, being the TG level superior. Both figures reach normal range after one year of GFD. Calculated LDL cholesterol figures show no difference with treatment. During challenge period, a decrease in HDL cholesterol is found, with no change in other studied parameters. Considering the intestinal mucosa an important step in absorption of TG and cholesterol, the origin of these alterations is probably multi factorial and conditioned by the decrease in intestinal lipase, Apo A1, ApoB 48 and the lack of intra-erythrocyte esterification . Behavior of HDL cholesterol in this sample follows the same pattern than in adults. 28. DOCOSAHEXAEONIC ACID AND/OR 5-METHYL-TETRAHYDROFOLATE NUTRITIONAL INTERVENTION DURING PREGNANCY AND LONG CHAIN POLYUNSATURATED FATTY ACIDS PLACENTAL TRANSPORT. INVEST NUTR ALIM PEDIATR (REV ON-LINE) 2004; 2. #30. HTTP:// WWW.SEINAP.ORG Campoy C1, Dolz V1, Marchal G2, Decsi T3, Gil A4, Linde J4, Jiménez M1, Molina Font JA1, Koletzko B5
1Dept. of Paediatrics. School of Medicine. University of Granada. Spain. 2Dept. of Obstetrics and Gynecology. Granada’s University Hospital San Cecilio. 3Dept. of Paediatrics, University of Pécs. Hungary. 4Dept. de Biochemistry and Molecular Biology. School of Pharmacy. University of Granada.
5Dr. v. Haunersches Kinderspital, LMU München. GermanyLarqué et al. (2003) have demonstrated that higher mother’s fatty acid (FA) concentrations in plasma than umbilical cord’s, determine a positive gradient of FA from mother to the foetus. Moreover, the placental tissue shows a preferential metabolic pathway to transfer docosahexaeonic acid (DHA) from mother to the foetus, in contrast to linoleic acid, oleic acid or palmytic acid. Some other studies have shown that the order for the fatty acid transport through the placenta to the foetus would be: DHA > α-linolenic acid> linoleic acid > oleic acid > arachidonic acid. So, a high long chain polyunsaturated fatty acid intake (LC-PUFAs) during pregnancy may improve an increase in the DHA concentrations of the foetal central nervous system. On the other hand, folic acid (FAc) has been shown to be able to improve the DHA bioavailability. A total of 155 Spanish healthy pregnant women participants in the NUHEAL study; aged between 18 and 40 years, were recruited at the 20±1 wks of gestation. Following a double blind & random design, were subdivided into 4 groups, depending on the supplement received until delivery (DHA: 0.5 g/day; 5-MTHF: 0.4 mg/day; both or placebo). In this study we try to analyse the influence of these supplements and the daily intake during pregnancy on the LC-PUFAs in the mother’s plasma phospholipids and in their neonates’. Methods: Plasma phospholipids’ LC-PUFAs were measured by gas chromatography. Individual questionnaires were done to evaluate the food daily intake in 24 hours at 20th
and 30th weeks of pregnancy. To transform the data into quantifiable data the Spanish tables (Novartis 1.7.01) for food composition were used. Statistical analysis: ANOVA, Lineal General Model for repeated measures and correlation study were done. *p<0.0001; #p<0.005; $p<0.03. Results: Following the Recommended Dietary Allowances (RDAs), the mother’s diet at 20th of pregnancy was rich in fat (92% of the mothers), proteins (96% of the subjects studied) and low in carbohydrates in the 78% of the mothers. The 60% of the mothers did not arise the RDAs for linoleic acid (13 g/day), nor for linolenic acid (93%) and the 55% of them did not achieve the RDAs for DHA (300 mg/day). The 97% of the pregnant women did not follow the RDAs for folic acid, and in the 73% the daily intake for folic acid was <0.4 mg/day. Lineal and direct correlations between DHA daily intake at 30th weeks of pregnancy and the EPA and DHA concentrations in the maternal plasma phospholipids at delivery (r:0.50*; r:0.37#). Daily DHA intake at 30th weeks of pregnancy was inversely correlated with AA/DHA and n-6/n-3 ratios of their neonates (r:-0.48*; r:-0.40#). Mother’s daily intake of FAc
had a significant influence on the n-3 LC-PUFAs in the neonates (r:0.30$). Moreover, significant correlations between mothers and their newborns were established regarding for instance DHA: r:0.30, p=0.0028; AA/DHA: r:-0.43, p<0.0001. The most important quantitatively n-3 LC-PUFAs found in the umbilical cord was DHA. Conclusions: Pregnant women’s LC-PUFAs intake is low in a high percentage of the mothers studied. A high consumption of FAc during pregnancy determines an increase in the LC-PUFAs of their neonates. The influences of the mother’s diet on the plasma phospholipids LC-PUFAs in their neonates are confirmed; so, an important role of the pregnant women’s diet and the placental metabolism intervention during critical periods of life are demonstrated.This work is a part of the 5th EU Framework Program (Research grant Nutrition and Healthy Lifestyle [NUHEAL], grant no. CLK1-CT-1999-00888). 29. LYSOSOMAL DISEASES : ENZYME REPLACEMENT THERAPY. INVEST NUTR ALIM
PEDIATR (REV ON-LINE) 2004; 2. #31. HTTP:// WWW.SEINAP.ORG J Dalmau Serra*, I Vitoria Miñana*** Nutrition and Metabolism Disorders Unit, Children’s Hospital La Fe. Valencia. Spain.**Pediatric Nutrition Unit. Lluis Alcanys Hospital. Xátiva. Spain.Lysosomes are cellular organelle rich in enzymes that degrade complex molecules. Genetic defects of these enzymes cause incompletely digested material to store, therefore generating functional disturbances of the affected cellular systems, mainly the connective and nervous tissues and the parenquimal organs. There are some 40 lysosomal diseases. Until now, the therapy has been accepted as palliative or partially effective. Since the introduction of the placenta-derived enzymatic preparations and, more recently, the enzyme synthesis with DNA-recombinant methods, we are able to start an enzyme replacement therapy (ERT) in some diseases: Gaucher, Mucopolysacchari-dosis I, Fabry, Pompe and Niemann-Pick B. Considering the relatively low number of patients susceptible to receivethe ERT, this treatment has been initiated without fulfilling the 4 clinical trial steps, therefore little information on its safety and efficacy is available.The experience about ERT in 2 types of diseases is described:
1. Gaucher disease type I : Three patients (2M, 1 F) were diagnosed between 2.5 and 4 years of age by means of the leukocytic enzymatic activity and mutation analysis. ERT was started in 2 patients in 1995 (8,4 and 10 year-old) and in 2002 the third one (2,7 year-old). Slight pancytopenia, large hepatomegaly (1,5-3 times the normal volume) and splenomegaly (10-30 times). One year after ERT was initiated (60 IU/2 weeks) pancytopenia normalized. The chitotriosidase levels decreased over 50 % during the first 2 years. Hepatomegaly has decreased 20-60 % and splenomegaly 75-85% over the 9 years of ERT. No side-effects were present. No antibodies were detected. ERT seems effective in Gaucher disease type I.
2. Mucopolysaccharidosis I (Hurler/Scheie) : 5 y-old, male, presenting dwarfism, facial coarsening, spasticity, slight aortic dysplasia and characteristic radiologic abnormalities; progressive asthenia developed, spasticity increased and intense dorsal pain appeared. His sister was diagnosed one year later, progressing in a similar way though in a lesser intensity. Tonsillectomized. IQ 87 and 100 respectively. Corneal opacities enlarging. Normal pulmonary capacity. Diagnosis was confirmed by determinig leukocyte α-idurodinase; no mutations identified. ERT initiated at 7 and 12 years, well tolerated. As there is no visceral enlargement and no biochemical marker is indicative of illness evolution, it is difficult to asses the degree of improvement achieved. ERT efficacy in this disease (assessed in adults by vital capacity and distance long walk in 6 minutes) seems encouraging, but there are no data in the mid term about its safety and effectiveness.
Commentaries : The presented data suggest that ERT is effective in the short/mid term, but there are many questions about its use: to individualize the indications (age, symptoms/signs, biochemical and Rx markers, social pressure etc), dose and their frequency, treatment-response approach (including quality of life), side-effects and safety and effectiveness in the long run. 30. ALLERGY AND NUTRITION. FACTS AND FANCIES. INVEST NUTR ALIM PEDIATR (REV ON-LINE) 2004; 2. #32. HTTP:// WWW.SEINAP.ORG Manuel Cruz, Barcelona.

The relation between food and allergy shows some controversial points with pure reality now overcoming the previously accepted myths. The first sign of evidence is the increase in the prevalence of allergy and asthma presently affecting 15% of the pediatric population. The next one is more complex due to a multifactor origin: genetics, environment, infections and nutrition. It has been currently admitted that the allergic predisposition could be weakened with breastfeeding owing to the milk's bio-active factors. However, there is evidence (1) that breastfeeding could be related to eczema and other allergies, for its content in alimentary antigens, RANTES, IL-4 and other cytokines. In this way this protective action could also be hampered by the content in breastmilk of pollutants, in addition to tobacco smoke (NAHNES III) and the fact of the real decrease in respiratory infections in the breastfed infant (2,3). Solid foods with their many diversities should be started at a later stage in order to prevent food allergy. The counterpart of this delay could be the lack of supply of polyunsaturated fatty acids (fish...) or antioxidant factors (fruit and vegetables). Long chain polyunsaturated fatty acids and their metabolic end products have a well known anti-inflammatory action by means of the inhibition of leukotrienes and prostaglandins (5). This action is clear on prevention grounds but not so in the therapeutic ones (6). Concerning the antioxidant factors (vitamins A,C,E, betacarotene, flavonoids) enough data exists in favour of their preventive and therapeutic action. Because of the parallel oxidative stress in the inflammatory process in asthma in particular and in allergy in general, this kind of stress would favour a greater inflammatory gene expression in the allergic subject (7,8). The role of minerals such as calcium, magnesium, selenium, zinc or copper has also been updated in its contribution to the allergic response. The interest for lipids is greater (9) because of the diet excess which would help obesity and also atopy. Concerning obesity there is abundant literature, sometimes controversial but with a predominant trend which shows an increase in severity and frequency of asthma (10). An eventual protective action of breastfeeding against obesity is also considered.
Probiotics. When administered earlier to the infant they could reduce the allergy incidence up to 50%. A certain protective action on digestive permeability, augmented in the asthmatic child, could be added to its claimed metabolic and immune qualities. In the binomial 'food-allergy' a better knowledge of alimentary antigens is important and particularly updating the diagnostic methods in order to distinguish the myths from reality. From a total of 28% of children with a suspected food allergy at a certain moment this allergy ascertained is only in 8% of infants, 2-3% in children and only in 1% in adolescents. Maturity factors, additives, food contaminating substances, immune response and the diagnostic guidelines could all affect these frequency rates (13): a raised specific IgE for some people can be as valuable as a provocative test and or instrumental study for others. In this way the interpretation of IgG antibodies variation so widely measured is more difficult too. In common clinical practice the attention should not be limited to the typical 'gastro-enteritis-urticaria-asthma crisis' but also to isolated cases of severe and unmanageable bronchial asthma. When considering the therapeutic approach the early hypo-allergenic formulas were a passing myth, giving way to the efficient elimination diets and the growing use of protein hydorlysates of very low molecular weight. Perhaps soya protein is still an alternative. Furthermore and with a broad mind one should not be limited only to the dietary aspects but also to the pathogenic condition (14) as well as the present and future therapy resources.
















![Home | Arabicfirst - Book of Countries · 2010. 8. 5. · Page 34Page 2 1. Where would you find the Pearl Monument? A. Bahrain [ ] B. Iraq C. England D. China [] [] [] 2. Where would](https://static.fdocuments.mx/doc/165x107/606a13650e45f536ff1d2599/home-arabicfirst-book-of-countries-2010-8-5-page-34page-2-1-where-would.jpg)