INMUNOTERAPIA ESPECÍFICA SUBLINGUAL - Alergomurcia especfica sublingual.pdf · Porcentaje de...
24
1 INMUNOTERAPIA ESPECÍFICA SUBLINGUAL Dr Adnan Tanovic Departamento Médico STALLERGENES-IPI, S.A. Noviembre 2005 Tratamiento óptimo de alergia incluye INMUNOTERAPIA ESPECIFICA (ITE) Alergia Inmunoterapia especifica (ITE) •Efectividad •Prescripción especialista •Altera curso natural de la enfermedad Medicación •Seguridad •Efectividad •Fácil administración Educación del paciente •Siempre indicada TRATAMIENTO OPTIMO Evitación de alergenos •Si es posible Noviembre 2005
Transcript of INMUNOTERAPIA ESPECÍFICA SUBLINGUAL - Alergomurcia especfica sublingual.pdf · Porcentaje de...

1
INMUNOTERAPIA ESPECÍFICA SUBLINGUALDr Adnan TanovicDepartamento MédicoSTALLERGENES-IPI, S.A.
Noviembre 2005
Tratamiento óptimo de alergia incluye INMUNOTERAPIA ESPECIFICA (ITE)
Alergia
Inmunoterapia especifica (ITE)•Efectividad•Prescripción especialista•Altera curso natural de la enfermedad
Medicación•Seguridad•Efectividad•Fácil administración
Educación del paciente•Siempre indicada
TRATAMIENTO OPTIMO
Evitación de alergenos•Si es posible
Noviembre 2005

2
PATOLOGIA ALERGICA
ALERGIA RESPIRATORIAASMA (3 -10% de la población)RINITIS (12-20% DE LA POBLACION)CONJUNTIVITIS OTITIS MEDIA SEROSA
ALERGIA HIMENOPTEROSREACCIONES TRAS PICADURA DE ABEJA Y AVISPA (Inoculación de veneno). “INMUNOTERAPIA EFECTIVA EN MAS DEL 90 % EN VESPIDOS Y 80% EN ABEJA”
ALERGIA AL LATEXALERGIA CUTANEA
URTICARIA Y/O ANGIOEDEMADERMATITIS ATOPICADERMATITIS DE CONTACTO
ALERGIA ALIMENTARIAALERGIA ALIMENTOSALERGIA A ADITIVOSINMUNOLÓGICAS: IGE MEDIADASNO INMUNOLÓGICAS: ENZIMATICO O FARMACOLÓGICO.
ALERGIA MEDICAMENTOS5-10 % DE LAS REACCIONES A MEDICAMENTOS SON DE NATURALEZA ALERGICA
INM
UN
OTE
RA
PIA
Noviembre 2005
Porcentaje (%)
0 10 20 30 40 50 60 70
Aler
geno
s
Polenes 60%
Ácaros 18%
Epitelio/pelo 12%
Heminopteros 5%
Alimentos 3%
Medicamentos 2%
PATOLOGIA ALERGICA
Noviembre 2005

3
Porcentaje (%)
0 10 20 30 40 50 60 70
Aler
geno
s
Polenes 60%
Ácaros 18%
Epitelio/pelo 12%
Heminopteros 5%
Alimentos 3%
Medicamentos 2%
PATOLOGIA ALERGICA
Noviembre 2005
"About the beginning or middle of June in every year ….. …. A sensation of heat and fulness isexperienced in the eyes ….
…. To this succeeds irritation of thenose producing sneezing ….
…. To the sneezings are added a further sensation of tightness of thechest, and a difficulty of breathing"
Primera descripción de la fiebre de henoJohn Bostock, Med Chir Trans London, 1819; 10: 161
Cada año al principio o mediados de junio…
…siento un enrogecimiento y lecrimeo en los ojos
A esto se añade la irritación nasal que me produce estornudos…
Al los estornudos se añade una “presion” en el pecho y dificultades de respirar …
Introdujo el termino de “Hay fiver”
Noviembre 2005

4
INMUNOTERAPIA ESPECIFICA“Vacunas terapéuticas para las enfermedades alérgicas”
1900 H.H. Curtis (extractos acuosos de polen).1911 Noon y Friedman: primeros resultados de la “Inoculación profiláctica” contra la fiebre del heno.1913 Weil introduce el término “Desensibilización ” .1922 Cook introduce el término de “Hiposensibilización”.1971 Norman y Lichtenstein cambio por Inmunoterapia Específica (ITE).1998 Artículo de opinión de la OMS.
HISTORIAL DE LA ITE
Noviembre 2005
“Allergen immunotherapy, when introduced at the onset or during the early phase of the disease, may modify the natural course of the allergic disease ”
Bousquet J, Lockey RF, Malling HJ. et al. Allergy 1998; 53.
« OMS / WHO Position Paper » sobre ITE
WHO 1998
5
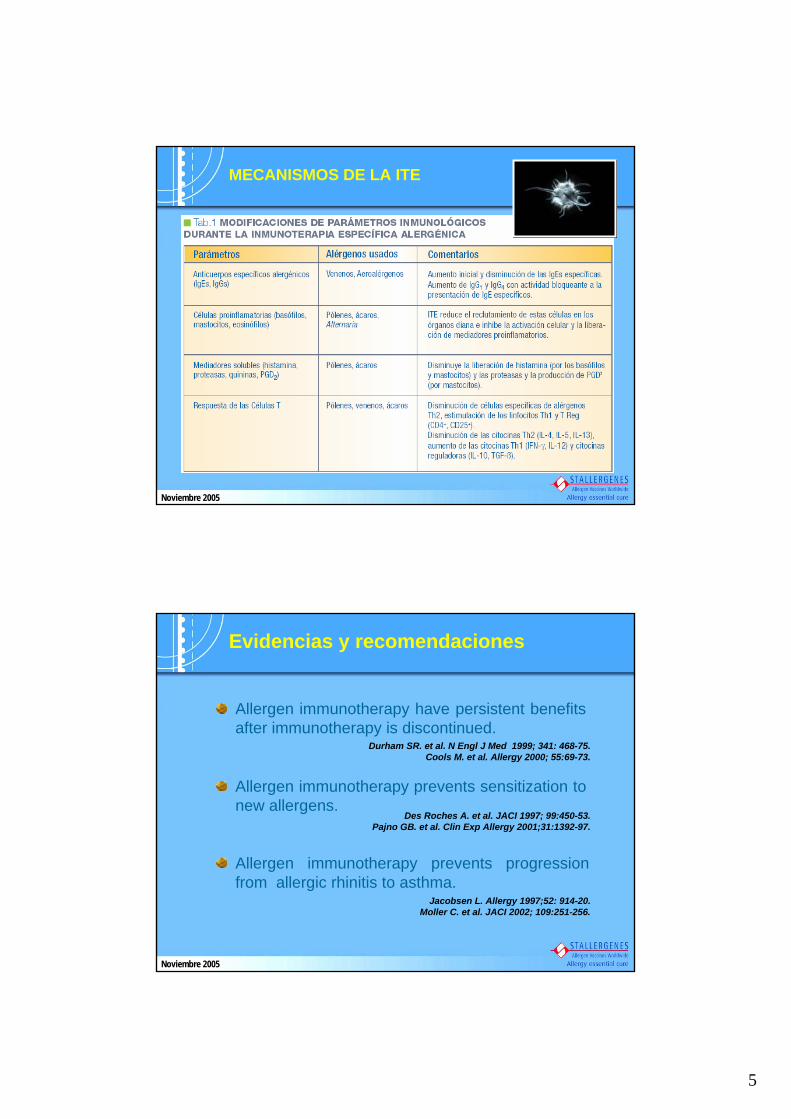
MECANISMOS DE LA ITE
Noviembre 2005
Allergen immunotherapy have persistent benefitsafter immunotherapy is discontinued.
Durham SR. et al. N Engl J Med 1999; 341: 468-75. Cools M. et al. Allergy 2000; 55:69-73.
Allergen immunotherapy prevents sensitization to new allergens.
Des Roches A. et al. JACI 1997; 99:450-53. Pajno GB. et al. Clin Exp Allergy 2001;31:1392-97.
Allergen immunotherapy prevents progression from allergic rhinitis to asthma.
Jacobsen L. Allergy 1997;52: 914-20.Moller C. et al. JACI 2002; 109:251-256.
Evidencias y recomendaciones
Noviembre 2005
6
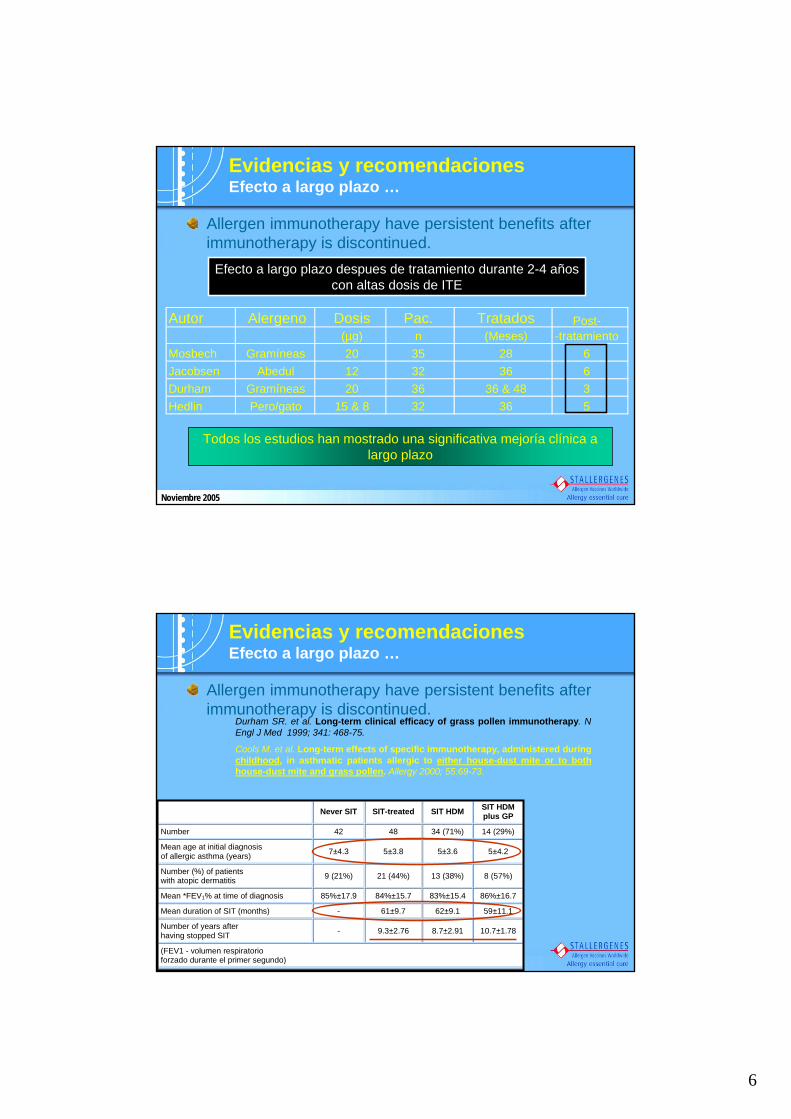
Allergen immunotherapy have persistent benefits after immunotherapy is discontinued.
Evidencias y recomendacionesEfecto a largo plazo …
Autor Alergeno Dosis Pac. Tratados(µg) n (Meses) -tratamiento
Mosbech Gramíneas 20 35 28 6Jacobsen Abedul 12 32 36 6Durham Gramíneas 20 36 36 & 48 3Hedlin Pero/gato 15 & 8 32 36 5
Post-
Efecto a largo plazo despues de tratamiento durante 2-4 años con altas dosis de ITE
Todos los estudios han mostrado una significativa mejoría clínica a largo plazo
Noviembre 2005
Never SIT SIT-treated SIT HDM SIT HDMplus GP
Number 42 48 34 (71%) 14 (29%)
Mean age at initial diagnosis of allergic asthma (years) 7±4.3 5±3.8 5±3.6 5±4.2
Number (%) of patients with atopic dermatitis 9 (21%) 21 (44%) 13 (38%) 8 (57%)
Mean *FEV1% at time of diagnosis 85%±17.9 84%±15.7 83%±15.4 86%±16.7
Mean duration of SIT (months) - 61±9.7 62±9.1 59±11.1
Number of years after having stopped SIT - 9.3±2.76 8.7±2.91 10.7±1.78
(FEV1 - volumen respiratorio forzado durante el primer segundo)
Allergen immunotherapy have persistent benefits after immunotherapy is discontinued.
Durham SR. et al. Long-term clinical efficacy of grass pollen immunotherapy. N Engl J Med 1999; 341: 468-75.
Cools M. et al. Long-term effects of specific immunotherapy, administered during childhood, in asthmatic patients allergic to either house-dust mite or to both house-dust mite and grass pollen. Allergy 2000; 55:69-73.
Evidencias y recomendacionesEfecto a largo plazo …

7
Never SIT SIT-treated SIT HDM SIT HDMplus GP
Number 42 48 34 (71%) 14 (29%)
Mean age at initial diagnosis of allergic asthma (years) 7±4.3 5±3.8 5±3.6 5±4.2
Number (%) of patients with atopic dermatitis 9 (21%) 21 (44%) 13 (38%) 8 (57%)
Mean *FEV1% at time of diagnosis 85%±17.9 84%±15.7 83%±15.4 86%±16.7
Mean duration of SIT (months) - 61±9.7 62±9.1 59±11.1
Number of years after having stopped SIT - 9.3±2.76 8.7±2.91 10.7±1.78
(FEV1 - volumen respiratorio forzado durante el primer segundo)
Allergen immunotherapy have persistent benefits after immunotherapy is discontinued.
Durham SR. et al. Long-term clinical efficacy of grass pollen immunotherapy. N Engl J Med 1999; 341: 468-75.
Cools M. et al. Long-term effects of specific immunotherapy, administered during childhood, in asthmatic patients allergic to either house-dust mite or to both house-dust mite and grass pollen. Allergy 2000; 55:69-73.
Evidencias y recomendacionesEfecto a largo plazo …
S IT treated(n=48)
C ontro ls(n=42) P
As thm atic com pla in ts 0 .0006
N ever 13 (27% ) 3 (7% )
Sporad ically 27 (56% ) 15 (36% )
Frequent 8 (17% ) 24 (57% )
Antias thm atic drugs 0 .38
N ever 22 (46% ) 12 (29% )
Sporad ically 14 (29% ) 16 (38% )
Frequent 12 (25% ) 14 (34% )
SP T w ith H D M extract (in m m )
4 .5±1 .72 5 .3±3.12 0 .17
FE V 1% 98±16.1% 105±15.4% 0 .06
Allergen immunotherapy prevents sensitization to new allergens.
Des Roches A. et al. Immunotherapy with a standardized Dermatophagoides pteronyssinus extract. VI. Specific immunotherapy prevents the onset of newsensitizations in children. JACI 1997; 99:450-53.
Pajno GB. et al. Prevention of new sensitizations in asthmatic childrenmonosensitized to house dust mite by specific immunotherapy. A six-year follow-up study.Clin Exp Allergy 2001;31:1392-97.
Evidencias y recomendacionesPrevención de nuevas sensibilizaciones …
•22 niños (<6 años) tratados con ITE,vs.•22 niños tratados con farmacoterapia (control) monosensibilizados a ácaros.
•Seguimiento durante 6 años…
Table I. Development of new sensitivities
New sensitivities Initial sensitivity No. of patients None Cat Dog Alt Grass
SIT group 22 10 6 4 2 1 Control group 22 0 12 8 6 6 Alt, Alternaria species.
Noviembre 2005

8
Allergen immunotherapy prevents progression fromallergic rhinitis to asthma.
Jacobsen L. Immunotherapy with partially purified and standardized tree pollenextracts. IV. Results from long-term (6-year) follow-up.Allergy 1997;52: 914-20.
Moller C. et al. Pollen immunotherapy reduces the development of asthma in children with seasonal rhinoconjunctivitis (the PAT-study).JACI 2002; 109:251-256.
Evidencias y recomendacionesProgresión de rinitis a asma…
Ningún paciente recibía tratamiento diario contra el asma
Noviembre 2005
Allergen immunotherapy prevents progression fromallergic rhinitis to asthma.
Jacobsen L. Immunotherapy with partially purified and standardized tree pollenextracts. IV. Results from long-term (6-year) follow-up.Allergy 1997;52: 914-20.
Moller C. et al. Pollen immunotherapy reduces the development of asthma in children with seasonal rhinoconjunctivitis (the PAT-study).JACI 2002; 109:251-256.
Evidencias y recomendacionesProgresión de rinitis a asma…
Ningún paciente recibía tratamiento diario contra el asma
ITE
% d
e pa
cien
tes
0
20
40
60
80
Control
n = 60
n = 19
n = 40
n = 32
Sin asmaCon asma
Porcentaje de niños sin y con asma 3 años después de recibir la ITE
Odds-ratio = 2.52(1.3 – 5.1)
Noviembre 2005
9
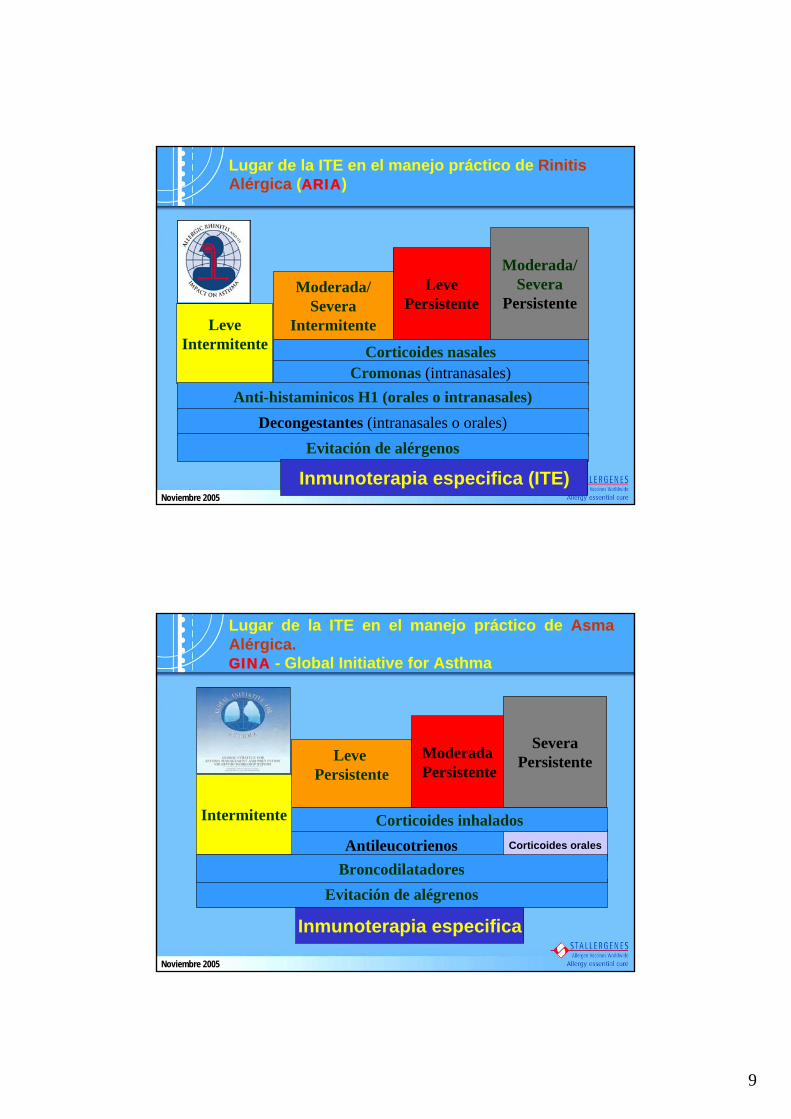
LeveIntermitente
Moderada/Severa
Intermitente
LevePersistente
Moderada/Severa
Persistente
Corticoides nasalesCromonas (intranasales)
Anti-histaminicos H1 (orales o intranasales)Decongestantes (intranasales o orales)
Evitación de alérgenos
Inmunoterapia especifica (ITE)
Lugar de la ITE en el manejo práctico de Rinitis Alérgica (ARIA)
Noviembre 2005
Leve Persistente
Moderada Persistente
SeveraPersistente
Antileucotrienos
Evitación de alégrenos
Inmunoterapia especifica
Corticoides orales
Lugar de la ITE en el manejo práctico de Asma Alérgica. GINA - Global Initiative for Asthma
Corticoides inhalados
Broncodilatadores
Intermitente
Noviembre 2005

10
SCIT
SLIT
ITE: VÍAS DE ADMINISTRACIÓN
SCIT SLIT
SCIT:Eficacia comprobada PERO riesgo de reacciones adversas.Necesidad de tener rutas más seguras y aceptables.
Noviembre 2005
¿CONDICIONES SLIT?
SLIT - Misma eficacia que SCITSLIT - Seguridad confirmadaSLIT - Rápidos iniciosSLIT - Mayor aceptación de pacientesSLIT - Sin nódulos S/C (20-30%)SLIT - Mayor precisión de dosisSLIT - Tratamiento en casa
De la Inmunoterapia Subcutánea a la Inmunoterapia Sublingual
Noviembre 2005

11
OMS Position Paper 1998EAACI Position Paper 1998
« Estudios debidamente controlados y bien diseñados que utilizan la inmunoterapia sublingual aportan pruebas
de que esta forma de terapia puede ser una alternativaviable a la terapia con inyecciones parenterales »
EAACI Position Paper 1993
« Se necesitan datos más concluyentes antes de recomendar la terapia sublingual como tratamiento habitual de los trastornos alérgicos »
¿POR QUÉ ADMINISTRAR IT SUBLINGUAL? Evolución
Noviembre 2005
ALLERGIC RHINITIS AND ITS IMPACT ON ASTHMAARIA (OMS) 2001
« La eficacia de la IT sublingual con dosis altas de alergeno (al menos 50 a 100 veces la dosis acumulada en
IT subcutánea) está documentada con estudios controlados en doble ciego contra placebo. Dosis
menores no son eficaces»
¿COMO ADMINISTRAR IT SUBLINGUAL?
Noviembre 2005

12
Dosis acumulada a final del primer aDosis acumulada a final del primer añño:o:
4717 4717 µµg de g de BetBet v 1 v 1 27 27 µµg de g de BetBet v1v1
Dosis sublingualDosis sublingual::x 175 dosis x 175 dosis subcutsubcutáánea nea
Pretratamiento n = 71
TratamientoAño 1
TratamientoAño 2
ITSL
ITSL
ITSL
ITSL
ITSL
ITSL
ITSC ITSC
ITSCITSC
ITSC ITSC
Grupo SublingualGrupo Sublingual
Grupo PlaceboGrupo Placebo
Duración del tratamiento: 24 meses
Rinoconjuntivitis alérgica al polen
de abedulGrupo SubcutGrupo Subcutááneoneo
Inclusión n = 89
Clinical efficacy of sublingual and subcutaneous birch pollen allergen-specific immunotherapy: a randomized, placebo-controlled, double-blind, double-dummy study. Khinchi MS, Puolsen LK, Carat F, André C, Hansen AB, Malling HJ. Allergy. 2004 Jan;59(1):45-53.
Inmunoterapia Sublingual vs. Subcutánea
Noviembre 2005
Sínt
omas
:
0
1
2
3
1 2 3 4 5 6 7 8 9Weeks
Sym
ptom
sco
re
0
400
800
1200
1600
2000
2400
Polle
n
PollenSLITSCITPlacebo
0
1
2
3
1 2 3 4 5 6 7 8 9Weeks
Sym
ptom
sco
res
0
400
800
1200
1600
2000
2400
Polle
n
PollenSLITSCITPlacebo
SLIT y SCIT: La misma eficacia
1er año de tratamientoEstación polinica - 1998
BaselineEstación polínica 1997
Inmunoterapia Sublingual vs. Subcutánea
p < 0.002p < 0.002Phostal S/C vs. Placebo
nsnsPhostal S/C vs. Staloral S/L
p < 0.02p < 0.002Staloral S/L vs. Placebo
SCORE MEDICACIÓNSCORE SÍNTOMAS
Noviembre 2005

13
y
Eficacia clínica demostrada en la rinitis alérgica al polen de abedul
- Disminución significativa de los síntomas- Disminución significativa de la medicación
Seguridad confirmada a dosis altas
Inmunoterapia Sublingual vs. Subcutánea
Noviembre 2005
La mucosa oral: “Un lugar seguro e inmunocompetente”
Noviembre 2005
14
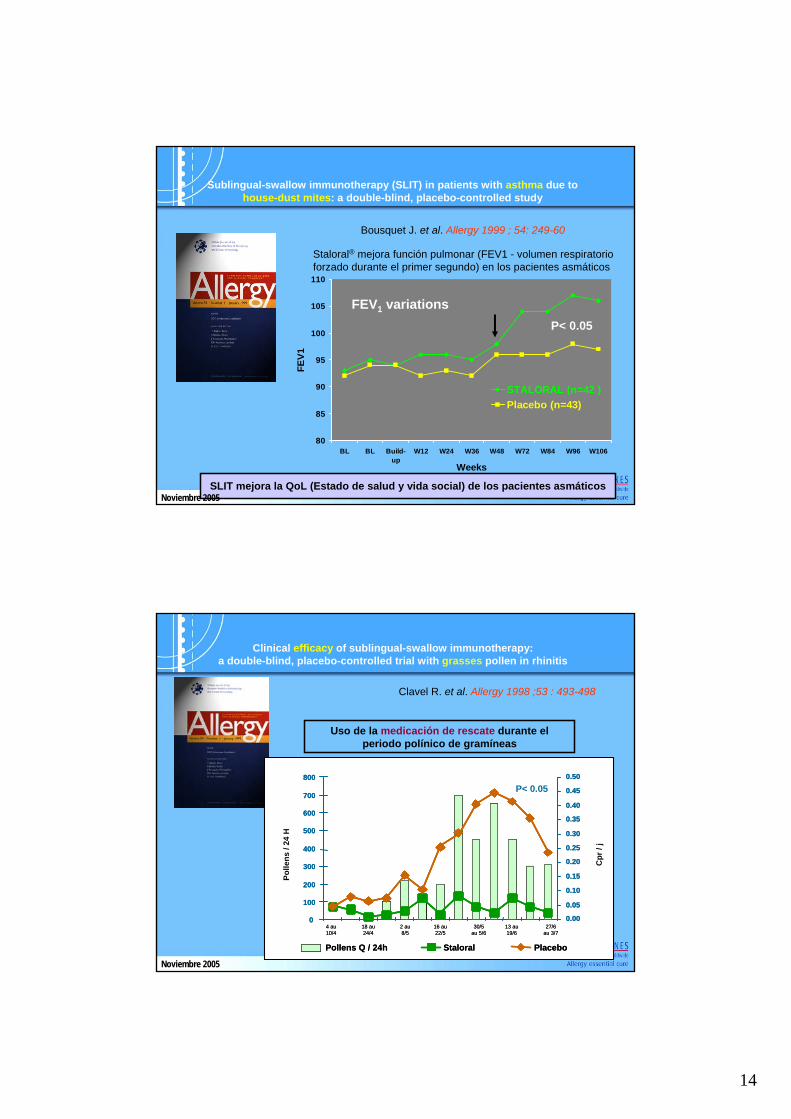
Sublingual-swallow immunotherapy (SLIT) in patients with asthma due to house-dust mites: a double-blind, placebo-controlled study
Bousquet J. et al. Allergy 1999 ; 54: 249-60
Staloral® mejora función pulmonar (FEV1 - volumen respiratorioforzado durante el primer segundo) en los pacientes asmáticos
80
85
90
95
100
105
110
BL BL Build-up
W12 W24 W36 W48 W72 W84 W96 W106
Weeks
FEV1
STALORAL (n=42 )Placebo (n=43)
FEV1 variations P< 0.05
SLIT mejora la QoL (Estado de salud y vida social) de los pacientes asmáticosNoviembre 2005
Clinical efficacy of sublingual-swallow immunotherapy: a double-blind, placebo-controlled trial with grasses pollen in rhinitis
Clavel R. et al. Allergy 1998 ;53 : 493-498
Uso de la medicación de rescate durante el periodo polínico de gramíneas
0
100
200
300
400
500
600
700
800
4 au10/4
18 au24/4
2 au8/5
16 au22/5
30/5au 5/6
13 au19/6
27/6au 3/7
0.00
0.05
0.10
0.15
0.20
0.25
0.30
0.35
0.40
0.45
0.50
Polle
ns /
24 H
Cpr
/ j
P< 0.05
Pollens Q / 24h Staloral Placebo
0
100
200
300
400
500
600
700
800
4 au10/4
18 au24/4
2 au8/5
16 au22/5
30/5au 5/6
13 au19/6
27/6au 3/7
0.00
0.05
0.10
0.15
0.20
0.25
0.30
0.35
0.40
0.45
0.50
Polle
ns /
24 H
Cpr
/ j
0
100
200
300
400
500
600
700
800
0
100
200
300
400
500
600
700
800
4 au10/4
18 au24/4
2 au8/5
16 au22/5
30/5au 5/6
13 au19/6
27/6au 3/7
4 au10/4
18 au24/4
2 au8/5
16 au22/5
30/5au 5/6
13 au19/6
27/6au 3/7
0.00
0.05
0.10
0.15
0.20
0.25
0.30
0.35
0.40
0.45
0.50
0.00
0.05
0.10
0.15
0.20
0.25
0.30
0.35
0.40
0.45
0.50
Polle
ns /
24 H
Cpr
/ j
P< 0.05
Pollens Q / 24h Pollens Q / 24h StaloralStaloral PlaceboPlacebo
Noviembre 2005
15
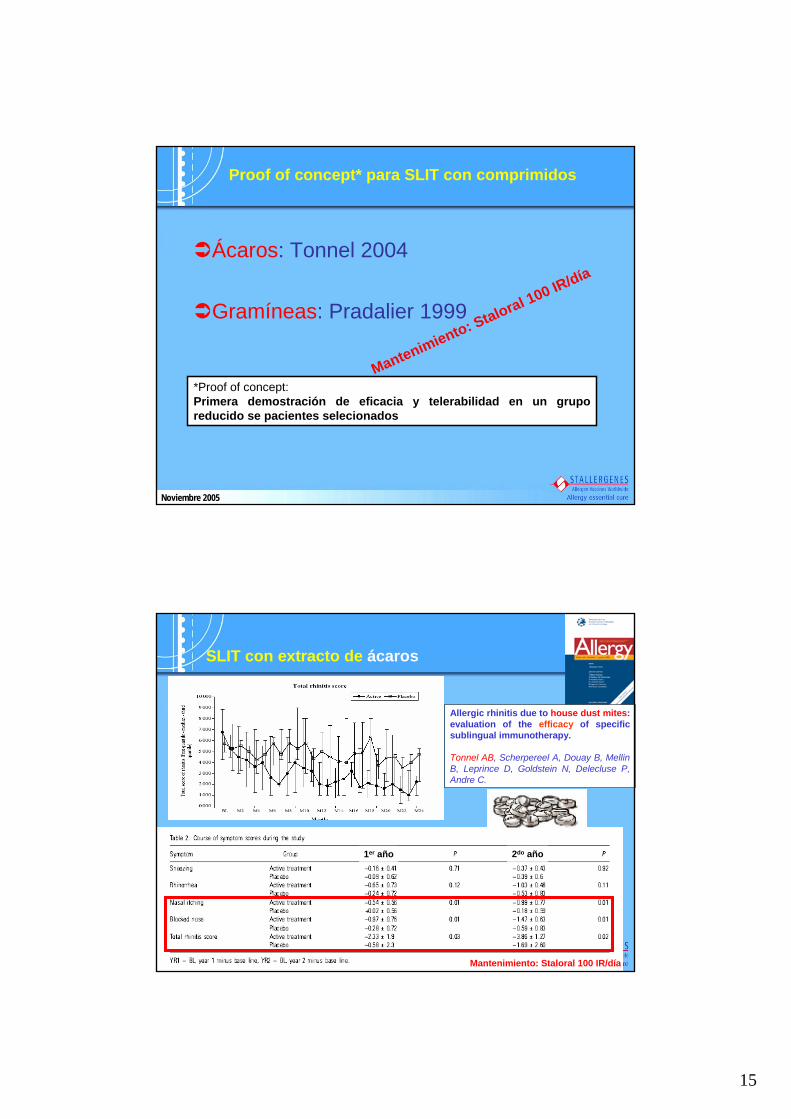
Proof of concept* para SLIT con comprimidos
Ácaros: Tonnel 2004
Gramíneas: Pradalier 1999
*Proof of concept:Primera demostración de eficacia y telerabilidad en un grupo reducido se pacientes selecionados
Mantenimiento: Staloral 100 IR/día
Noviembre 2005
SLIT con extracto de ácaros
Allergic rhinitis due to house dust mites: evaluation of the efficacy of specificsublingual immunotherapy.
Tonnel AB, Scherpereel A, Douay B, MellinB, Leprince D, Goldstein N, Delecluse P, Andre C.
Mantenimiento: Staloral 100 IR/día
1er año 2do año

16
Sublingual-swallow immunotherapy (SLIT) with a standardized five-grass-pollenextract (drops and sublingual tablets) versus placebo in seasonal rhinitis.Pradalier A et al. Allergy. 1999 Aug;54(8):819-28.
SLIT con extracto de gramíneas
Total conjunctivitis symptom score Number of days with asthmaTotal conjunctivitis symptom score Number of days with asthmaTotal conjunctivitis symptom score Number of days with asthma
En pacientes alérgicos al polen de gramíneas, los comprimidos (100 IR/día) han demostrado reducir la incidencia de
conjuntivitis en un 30% y un 50% en asma.Noviembre 2005
Seguridad de la SLIT
Safety of various dosage regimens during induction of sublingual immunotherapy. A preliminary study.
Grosclaude M et al, Int Arch Allergy Immunol. 2002 Nov;129(3):248-53Alergenos: 5 gramíneas
4 brazos: 3 niveles de inicio con comprimidos + placebo
17
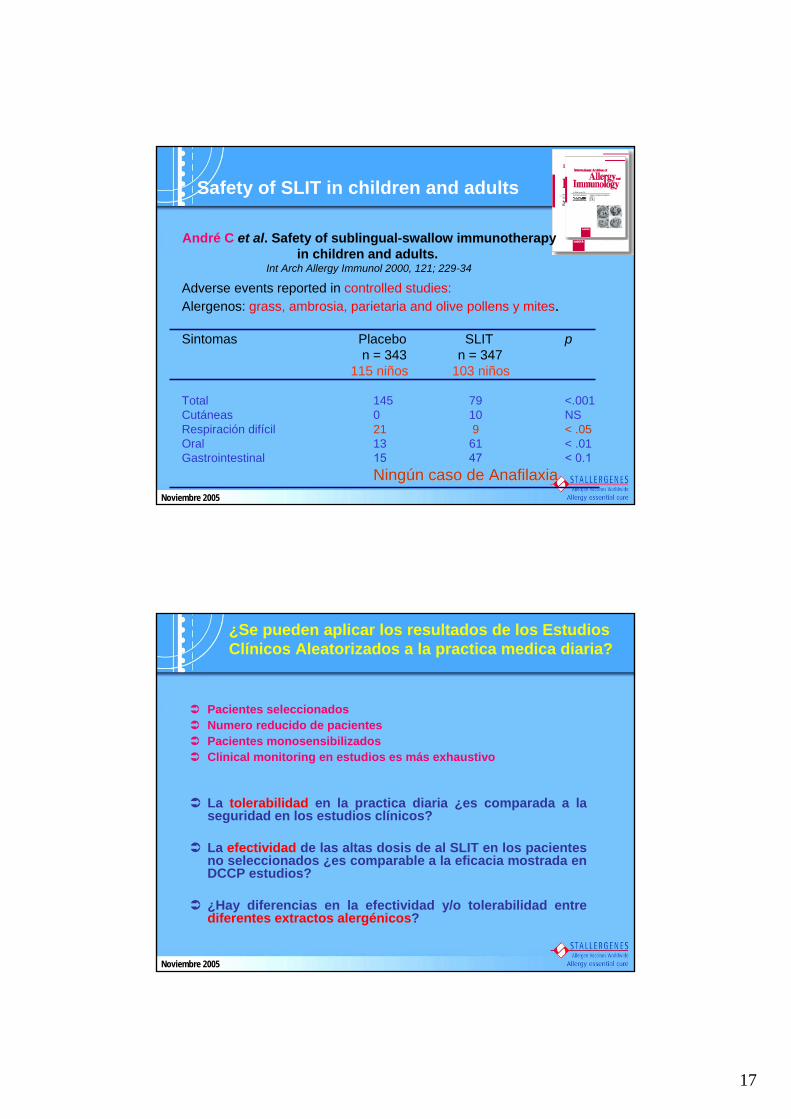
Safety of SLIT in children and adults
André C et al. Safety of sublingual-swallow immunotherapyin children and adults.
Int Arch Allergy Immunol 2000, 121; 229-34
Adverse events reported in controlled studies: Alergenos: grass, ambrosia, parietaria and olive pollens y mites.
Sintomas Placebo SLIT pn = 343 n = 347
115 niños 103 niños
Total 145 79 <.001Cutáneas 0 10 NSRespiración difícil 21 9 < .05Oral 13 61 < .01Gastrointestinal 15 47 < 0.1
NingNingúún caso de Anafilaxian caso de AnafilaxiaNoviembre 2005
¿Se pueden aplicar los resultados de los Estudios Clínicos Aleatorizados a la practica medica diaria?
La tolerabilidad en la practica diaria ¿es comparada a la seguridad en los estudios clínicos?
La efectividad de las altas dosis de al SLIT en los pacientes no seleccionados ¿es comparable a la eficacia mostrada en DCCP estudios?
¿Hay diferencias en la efectividad y/o tolerabilidad entre diferentes extractos alergénicos?
Pacientes seleccionadosNumero reducido de pacientesPacientes monosensibilizadosClinical monitoring en estudios es más exhaustivo
Noviembre 2005

18
Safety of SLIT in children and adults
Di Rienzo V, Pagani A, Parmiani S, Passalacqua G, Canonica GW.
POST-MARKETING SURVEILLANCE STUDY ON THE SAFETY OF SUBLINGUAL IMMUNOTHERAPY IN PEDIATRIC PATIENTS.
Allergy. 1999 Oct;54(10):1110-3268 niños; edad: 2-15 años
Noviembre 2005
Safety of SLIT in children and adults
Di Rienzo V, Pagani A, Parmiani S, Passalacqua G, Canonica GW.
POST-MARKETING SURVEILLANCE STUDY ON THE SAFETY OF SUBLINGUAL IMMUNOTHERAPY IN PEDIATRIC PATIENTS.
Allergy. 1999 Oct;54(10):1110-3268 niños; edad: 2-15 años
Noviembre 2005
19
Metaanálisis: Sublingual immunotherapy for allergic rhinitis - 2003 (Clinical Based Evidence: 1a)
« La IT sublingual es un tratamiento seguro que reduce significativamente los síntomas y la medicación en rinitis
alérgica»Wilson D.R, Torres Lima M, Durham S.R. Sublingual immunotherapy for allergic rhinitis (Cochrane Review). The Cochrane Library, Issue 2, 2003.
¿POR QUÉ ADMINISTRAR IT SUBLINGUAL?
Noviembre 2005
Metaanálisis con:979 patientes
21 estudios a doble ciego contra placebo
4 estudios seleccionados sólo con niños
3 estudios seleccionados con comprimidos
4 estudios seleccionados con pauta de inicio “rush”
Metaanálisis: Sublingual immunotherapy for allergic rhinitis- 2003 (Clinical Based Evidence: 1a)
« La IT sublingual es un tratamiento SEGURO que reduce significativamente los síntomas y la medicación en rinitis
alérgica»
¿POR QUÉ ADMINISTRAR IT SUBLINGUAL?
Noviembre 2005

20
4 días-11 díasRush(Días)
3h 30 min.-1.5 hUltra-rush(Horas)
3 semanas2 semanas-Cluster(Semanas)
13 semanas13 semanas3 semanasConvencional(Semanas-Meses)
VenenosSCITSLITPROTOCOLOS DE INICIO
¿Qué pauta de inicio en SLIT y SCIT?Caso Stallegenes
Noviembre 2005
Concentraciones disponibles:
Presentación:• Caja de inicio: frascos de 10 ml de 10 IR/ml y 300 IR/ml• Caja de mantenimiento: 2 ó 3 frascos de 10 ml de 300 IR/ml
Suspensión acuosa de administración sublingualExcipientes: Cloruro de sodio, glicerol, agua purificada
Vía sublingual
Noviembre 2005

21
Pautas de administración
1 presión = 0.1 ml
24 aplicaciones / semana = 2.4 ml
1 frasco 300 IR/ml = 1 mes
Caducidad = 12 meses
Fase de mantenimiento: concentración 300 IR/ml
Dosis mínima recomendada (24 aplicaciones / semana):8 aplicaciones 3 veces / semana
Vía sublingual
Noviembre 2005
1 presión = 0.1 ml (± 2%)
Vía sublingual
1 aplicación = 0.05 ml
Noviembre 2005

22
Concentraciones disponibles:•El frasco nº 1 bajo la solicitud expresa del médico para pacientes muy sensibles
Presentación:• Caja de inicio: 4 frascos de 10 ml de (0.1) - 1 - 10 - 100 IR/ml o IC/ml• Caja de mantenimiento: 1 ó 2 frascos de10 ml de 100 IR/ml o IC/ml
Suspensión acuosa de administración sublingualExcipientes: Cloruro de sodio, glicerol, agua purificada
Vía sublingual
Noviembre 2005
Pauta de inicio: Número de gotas por día
Pauta de mantenimiento:• La posología recomendada es de 20 gotas 3 veces / semana.
1 gota = 0.05 ml
3x 20 gotas / semana = 3 ml
1 frasco 100 IR/ml = 3 semanas
Caducidad = 12 meses
Vía sublingual
Noviembre 2005

23
Últimas noticias: Adherencia al tratamiento (estudio INSIT)American Academy of Allergy, Asthma and Immunology 2005 (AAAI), 8th – 22nd March, San Antonio
Lombardi C et al. Quantitative assessment of the adherence to alergoide sublingual immunotherapy in patients with dust house mite sensitization: The INSIT study. JACI; S140: 458
Estudio multicéntrico para evaluar la adherencia al tratamiento SLIT en comprimidos
• Entrevistas telefónicas (evaluación de numero de comprimidos restantes) durante 1er año de tratamiento,• 41 pacientes (15-65 años; 19: rinoconjuntivitis y 22: RC + asma),
• Adherencia: 3929 de 4056 comprimidos (96.8%)• Dosis esporádicamente olvidadas*: 14.6% pacientes* 1 comprimido al mes
Very satisfactory results in spite of fact to be
self-administrated
Noviembre 2005
METODOS:
Objetivo: El impacto de un tratamiento ITE (de 3 a 4 años, Stallergenes) versus farmacoterapia
Alérgenos: Dos tipos de alérgenos que causan principalmente manifestaciones respiratorias (rinitis alérgica y/o asma): pólenes y ácaros
Duración: 6 años para adultos y de 7 años para niños.
RESULTADOS:
Tratamiento coste global (costes directos + costes indirectos) eran 1.546 €ITE versus 1.769 € tratamiento con farmacoterapia.
Desde el punto de vista del seguro médico y teniendo en cuenta el coste por enfermedad asmática evitada, se ha notificado una reducción de 0.78 €/día durante el periodo de 6-7 años despues del tratamiento con la ITE.
Últimas noticias: Farmacoeconomía Annie Chicoye - Aremis consultants (Francia); Submitted for publication
Noviembre 2005

24
2. ComprimidosEstudios clínicos
3. Alergenos recombinantesAlergenos mayores seleccionadosEstudios preclínicos y clínicos
1. EstandarizacionesCaracterización de nuevos
extractos biológicos
Nuevos horizontes
Noviembre 2005
Extracto natural :Mezcla de proteínas sin purificar
Alergenos
recombinantes
SCIT SLIT
Comprimido alergenos mayoritarios
SLIT COMPRIMIDOS
Comprimidos extracto natural
Innovación : Comprimidos Alergenos mayoritarios recombinantes
Principioactivo
Forma galénica
Proyecto alergenos recombinantes y comprimidos
Noviembre 2005