Dr. Jacob Sellarés · Feb 15;142(4):233-9. APOYO PSICOLÓGICO TRATAMIENTO FARMACOLÓGICO...
48
Tabac i malalties pneumològiques Dr. Jacob Sellarés Servei de Pneumologia Institut del Tòrax Hospital Clínic
Transcript of Dr. Jacob Sellarés · Feb 15;142(4):233-9. APOYO PSICOLÓGICO TRATAMIENTO FARMACOLÓGICO...

Tabac i malalties pneumològiques
Dr. Jacob Sellarés
Servei de PneumologiaInstitut del TòraxHospital Clínic

El tabaquismo es una enfermedad adictiva crónicaque en más del 80 % de los casos se inicia antes de los 18años de edad y que produce muerte prematura a más de lamitad de aquellos que lo padecen, a través de enfermedadescardiovasculares, pulmonares y tumorales.

¿Qué hay en un cigarrillo?• El humo del tabaco contiene ≥4000 sustancias químicas, de
las cuales ≥250 son tóxicas o cancerígenas1
• La nicotina es adictiva, pero no cancerígena 3
• Fumar cigarrillos bajos en nicotina y alquitrán no supone un beneficio para la salud4
Sustancias químicas en el humo del tabaco2 Presentes también en …
Acetona QuitaesmalteButano Líquido volátilArsénico Veneno para hormigasCadmio Baterias de cochesMonóxido de carbono Humos del tubo de escapeTolueno Disolvente industrial
1. National Toxicology Program. 11th Report on Carcinogens; 2005. Available at: http://ntp‐server.niehs.nih.gov. 2. Mackay J, Eriksen M. The Tobacco Atlas. World Health Organization; 2006. 3. Harvard Health Letter. May 2005. 4. Surgeon General’s Report. The Health Consequences of Smoking; 2004.

Tabaquismo y enfermedades respiratorias
• EPOC
• Cáncer de pulmón
• Asma bronquial
• Infección respiratoria
• TBC
• Enfermedades intersticiales
• SAHS

EPOC y tabaquismo

La inhalación de los componentes del humo del tabaco constituyen el principal factor etiológico para el desarrollo de la EPOC

1) Enfermedades Respiratorias: son la tercera causa demortalidad después de los tumores y enfermedades delaparato circulatorio
2) EPOC en mayores 45 años: 9%
3) EPOC en mayores 65 años: 20%
4) EPOC: 410.000 altas / 3.097.000 estancias
Visión general del problema
ENS DE 2006:
Fuman 10 millones: 29 % edad > 15 años

lobal Initiative for Chronicbstructiveungisease
GOLD

Definition of COPD
COPD is a preventable and treatable disease with some significant extrapulmonary effects that may contribute to the severity in individual patients.
Its pulmonary component is characterized by airflow limitation that is not fully reversible.
The airflow limitation is usually progressive and associated with an abnormal inflammatory response of the lung to noxious particles or gases.

Classification of COPD Severityby Spirometry
Stage I: Mild FEV1/FVC < 0.70 FEV1 > 80% predicted
Stage II: Moderate FEV1/FVC < 0.7050% < FEV1 < 80% predicted
Stage III: Severe FEV1/FVC < 0.7030% < FEV1 < 50% predicted
Stage IV: Very Severe FEV1/FVC < 0.70FEV1 < 30% predicted or
FEV1 < 50% predicted pluschronic respiratory failure

IV: Very SevereIII: SevereII: ModerateI: Mild
Therapy at Each Stage of COPD*
FEV1/FVC < 70%
FEV1 > 80% predicted
FEV1/FVC < 70%
50% < FEV1 < 80%predicted
FEV1/FVC < 70%
30% < FEV1 < 50% predicted
FEV1/FVC < 70%
FEV1 < 30% predicted
or FEV1 < 50% predicted plus chronic respiratory failure
Add regular treatment with one or more long-acting bronchodilators (when needed); Add rehabilitation
Add inhaled glucocorticosteroids if repeated exacerbations
Active reduction of risk factor(s); influenza vaccinationAdd short-acting bronchodilator (when needed)
Add long term oxygen if chronic respiratory failure. Consider surgical treatments
*Postbronchodilator FEV1 is recommended for the diagnosis and assessment of severity of COPD

Burden of COPD: Key Points
• COPD is a leading cause of morbidity and mortality worldwide and results in an economic and social burden that is both substantial and increasing.
• COPD prevalence, morbidity, and mortality vary across countries and across different groups within countries.
• The burden of COPD is projected to increase in the coming decades due to continued exposure to COPD risk factors and the changing age structure of the world’s population.

Prevalence of GOLD Stage II & III in 12 Countries by Sex & Descending Prevalence of Smoking
(Lancet,2007; 370: 741-50)
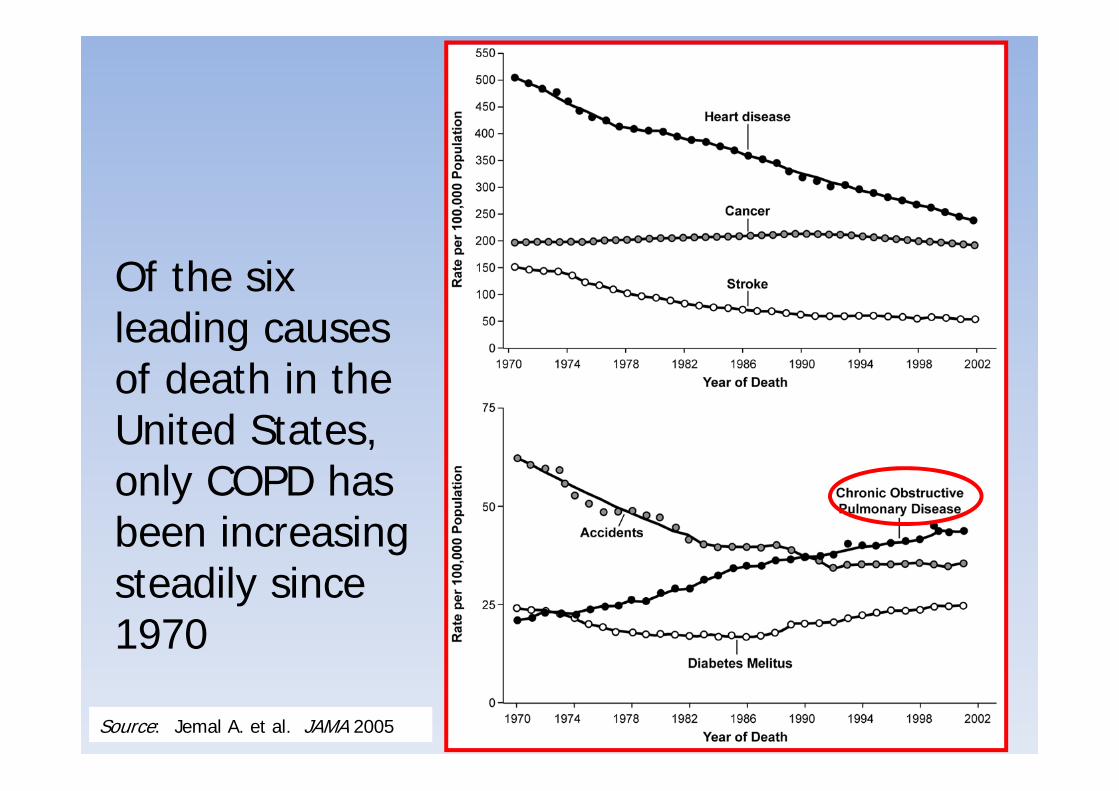
Of the six leading causes of death in the United States, only COPD has been increasing steadily since 1970
Source: Jemal A. et al. JAMA 2005

Miravitlles M, et al. Thorax 2009; 64:863-8
EPISCAN
10.2%40-80 años
1
11
2
-
OviedoBurgos
Vic
Sevilla
BarcelonaMadrid (2)
Córdoba
Huesca
Requena
Vigo
Sobradillo V, et al. Chest 2000; 118: 981-9
IBERPOC
1
11
2
-
Oviedo
Burgos
Cáceres
Vizcaya
Sevilla
ManlleuMadrid
Prevalencia de la EPOC en España
9.1%40-69 años

Risk Factors for COPD
Nutrition
Infections
Socio-economic status
Aging Populations

Espirometría en A.P.
Formación
Divulgación
IBERPOC(1997)
78%
EPISCAN(2007)
73%
Infradiagnóstico en la EPOC Evolución en España

No se puede mostrar la imagen. Puede que su equipo no tenga suficiente memoria para abrir la imagen o que ésta esté dañada. Reinicie el equipo y, a continuación, abra el archivo de nuevo. Si sigue apareciendo la x roja, puede que tenga que borrar la imagen e insertarla de nuevo.
LUNG INFLAMMATION
COPD PATHOLOGY
Oxidativestress Proteinases
Repair mechanisms
Anti-proteinasesAnti-oxidants
Host factorsAmplifying mechanisms
Cigarette smokeBiomass particles
Particulates
Source: Peter J. Barnes, MD
Pathogenesis of COPD

Mast cell
CD4+ cell(Th2)
Eosinophil
Allergens
Ep cells
ASTHMA
BronchoconstrictionAHR
No se puede mostrar la imagen. Puede que su equipo no teng
Alv macrophageEp cells
CD8+ cell(Tc1)
Neutrophil
Cigarette smoke
Small airway narrowingAlveolar destruction
COPD
Reversible IrreversibleAirflow Limitation
Source: Peter J. Barnes, MD

Four Components of COPD Management
1. Assess and monitor disease
2. Reduce risk factors
3. Manage stable COPDEducationPharmacologicNon-pharmacologic
4. Manage exacerbations

COPD and Co-Morbidities
COPD patients are at increased risk for: • Myocardial infarction, angina
• Osteoporosis
• Respiratory infection
• Depression
• Diabetes
• Lung cancer

COPD and Co-Morbidities
COPD has significant extrapulmonary
(systemic) effects including:
• Weight loss
• Nutritional abnormalities
• Skeletal muscle dysfunction

Management of Stable COPD
Reduce Risk Factors: Key Points
Reduction of total personal exposure to tobacco smoke, occupational dusts and chemicals, and indoor and outdoor air pollutants are important goals to prevent the onset and progression of COPD.
Smoking cessation is the single most effective — and cost effective — intervention in most people to reduce the risk of developing COPD and stop its progression (Evidence A).
Management of Stable COPD
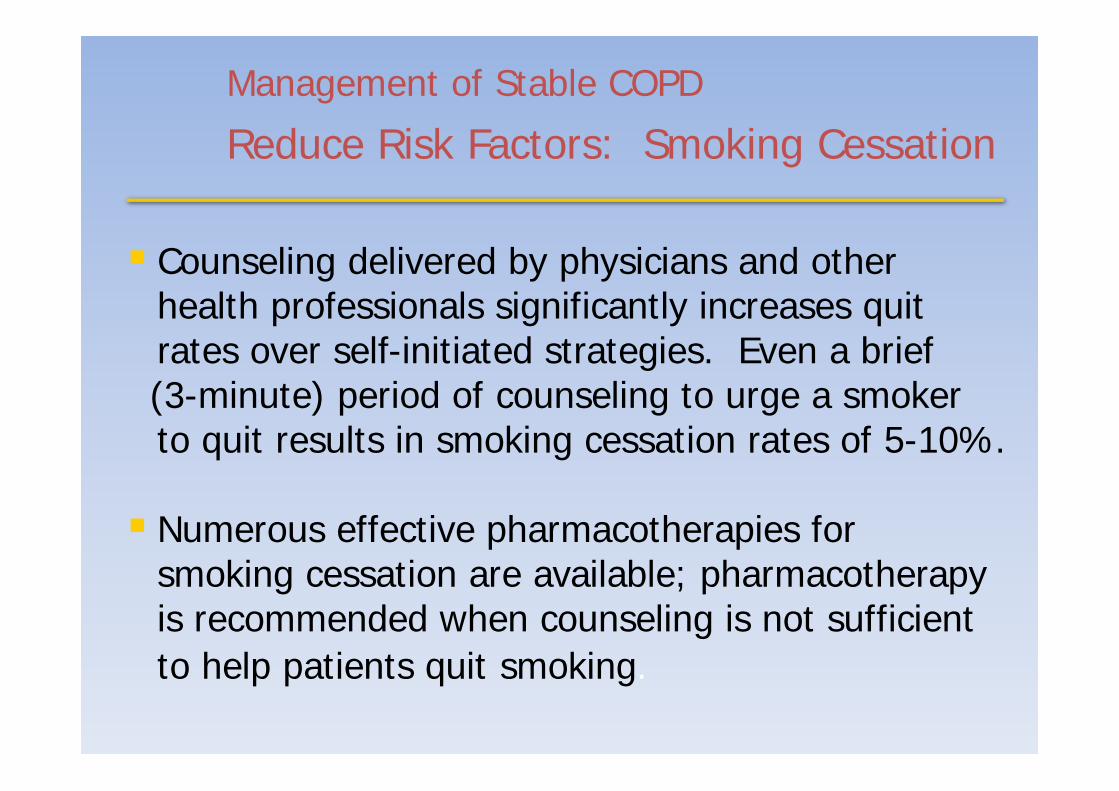
Reduce Risk Factors: Smoking Cessation
Counseling delivered by physicians and other health professionals significantly increases quit rates over self-initiated strategies. Even a brief (3-minute) period of counseling to urge a smoker to quit results in smoking cessation rates of 5-10%.
Numerous effective pharmacotherapies for smoking cessation are available; pharmacotherapy is recommended when counseling is not sufficient to help patients quit smoking.

Características diagnósticas del tabaquismo en fumadores-EPOC
Mayor inhalación y depósito de sustancias tóxicas del humo del tabaco
Mayor grado de dependencia física
IBERPOC: 30% Fagerström > 7
Mayor índice de comorbilidad psiquiátrica
Diferentes grados de motivación
Niveles más altos de CO en aire espirado
0
10
20
30
40
50
60
70
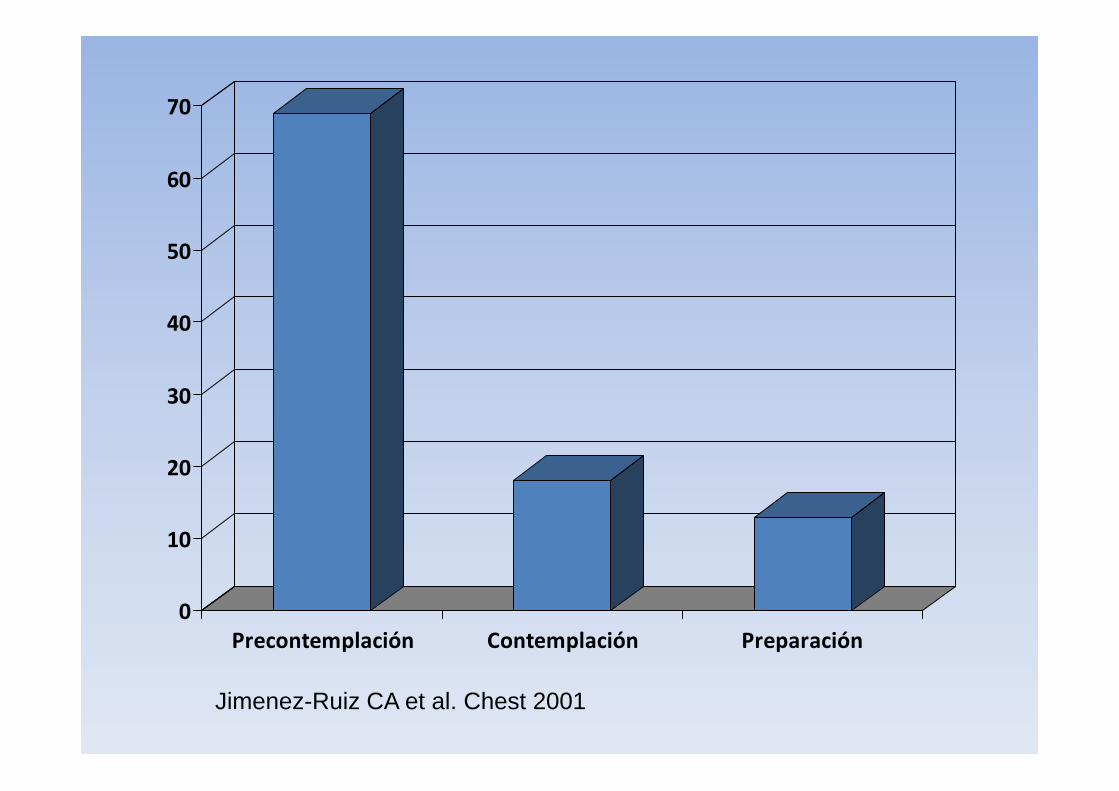
Precontemplación Contemplación Preparación
Jimenez-Ruiz CA et al. Chest 2001

ON SÓN ELS FUMADORS DEL NOSTRE VOLTANT?
Font: Becoña, 2004

Pérdida acelerada de la función pulmonar
Adaptado de Fletcher C & Peto R. BMJ 1977 con permisos
100
FEV1 (% del valor a los 25 años)No fumador o no Susceptible de fumar
Dejar de fumar a los 65 años
Dejar de fumar a los 45 años
Fumador habitual y susceptible de sus efectos
75
50
0
25
25 50 75
Edad (Años)
Invalidez
Muerte

Anthonisen NR et al. Am J Respir Crit Care Med 2002

Anthonissen NR et al. Ann Intern Med. 2005 Feb 15;142(4):233-9.


APOYO PSICOLÓGICO
TRATAMIENTO FARMACOLÓGICO
Tratamiento

Explicar estrecha relación: Tabaco-EPOC
Explicar la necesidad de dejar el tabaco como única medida eficaz
Indicar el empeoramiento si continúa fumando a pesar del tratamiento broncodilatador

Fármacos en el tratamiento del tabaquismo
• TSN– Sístemas de liberación agudos
• Chicles de nicotina• Comprimidos para chupar• Spray nasal *• Inhalador *
– Sistemas de liberación sostenida• Parches de nicotina
• Antidepresivos– Bupropion
• Vareniclina
* No comercializados en España

EPOC y tratamiento farmacológico tabaquismo
Seguimiento Abstinencia (%) Control (%)
TSN 5 años
11 años
6 meses
35
21.9
17
9
6
10
Bupropion 6 meses
1 año
1 año
6 meses
16
10
19
27.3
9
8.
9.
8.3
Vareniclina 6 meses‐1 año
25.8‐18.6 7.2‐5.6

TABLA 2 . Muertes atribu ibles al con sum o de tabaco, según causa y sexo. Españ a1998 (m odificada de Ban egas JR et al.9)
Causas de m uerte Total n º (% ) Varon es n º (% ) M ujeres n º (% )
Tu m ores m align os 22.040 (39,7) 20.932 (40,7) 1.108 (26,5)Labio, boca, farin ge 1.779 (3,2) 1.696 (3,3) 83 (2,0)Esófago 1.321 (2,4) 1.257 (2,4) 64 (1,4)Pán creas 691 (1,2) 559 (1,2) 132 (3,2)Larin ge 1.435 (2,6) 1.406 (2,7) 29 (0,7)Tráquea, bron qu ios,pu lm on es 14.664 (26,5) 14.001 (27,2) 663 (15,9)Cu ello de ú tero 81 (0,1) 0 81 (1,9)Vejiga 1.501 (2,7) 1.461 (2,8) 40 (1,0)Riñ ón 568 (1,0) 552 (1,1) 16 (0,4)
En ferm edadescard iovascu lares 20.097 (36,1) 18.213 (35,4) 1.885 (45,1)
Cardiopat ía isquém ica 7.116 (12,8) 6.548 (12,7) 569 (13,6)Otras cardiacas 5.300 (9,5) 4.724 (9,2) 576 (13,8)Cerebrovascu lares 5.103 (9,2) 4.557 (8,9) 546 (13,1)Otras circu latorias 2.578 (4,6) 2.384 (4.6) 194 (4,6)
En ferm edades resp iratorias: 13.475 (24,2) 12.286 (23,9) 1.189 (29,4)EPOC 11.629 (20,9) 10.626 (20,7) 1.004 (24.0)Otras resp iratorias 1.846 (3,3) 1.660 (3,2) 185 (4,4)
Total 55.613 (100) 51.431 (100) 4.182 (100)

Cáncer de pulmón
• El tabaco es el factor etiológico más importante en el desarrollo de cáncer de pulmón.
• Continuar fumando tras el diagnostico:– incrementa el riesgo de padecer un segundo tumor.
– aumenta la frecuencia de infecciones
– aumenta efectos secundarios de los tratamientos
– incrementa el riesgo quirúrgico
– disminuye la supervivencia.


Asma bronquial
• Se relaciona con:– broncoespasmo
– mayor frecuencia de crisis
– mayor gravedad de las crisis
= peor control del asma
• Mayor necesidad de tratamiento inhalado.

Asma bronquial

Infecciones respiratorias
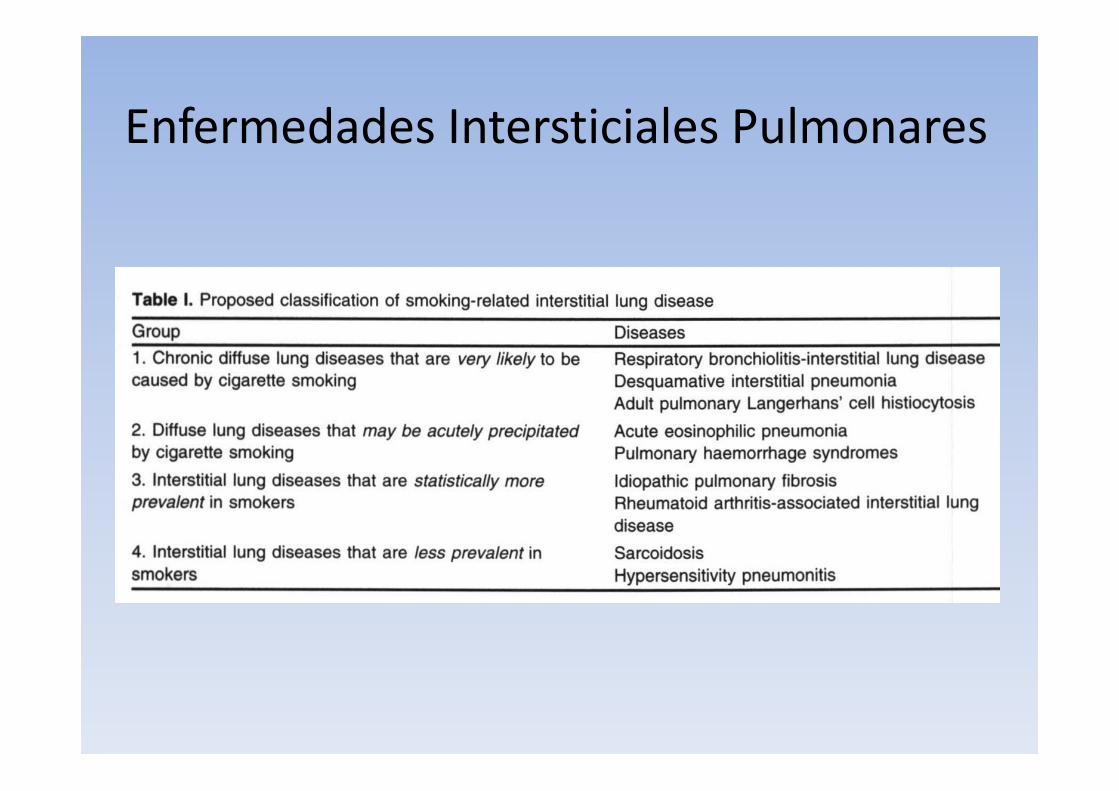
Enfermedades Intersticiales Pulmonares

Malalties Intersticials Pulmonars

SAHS y tabaquismo

SAHS y tabaquismo

SAHS y tabaquismo

CONCLUSIONES
• El tabaco es un factor causante o agravante de las principales enfermedades respiratorias crónicas.
• EL diagnóstico y tratamiento del tabaquismo debería ser incluido dentro de los procedimientos de rutina de intervención en los enfermos respiratorios.

Muchas gracias