Clinico social case Presentation
60
CLINICO-SOCIAL CASE PRESENTATION University of Medicine (1), Yangon PSM Posting Group 5, Sub-group A Roll No. 1 – 30
-
Upload
kyaw-san-lin -
Category
Health & Medicine
-
view
1.435 -
download
2
Transcript of Clinico social case Presentation
CLINICO-SOCIAL CASE PRESENTATION
University of Medicine (1), Yangon
PSM Posting Group 5, Sub-group A
Roll No. 1 – 30
FOR THIS CLINICO-SOCIAL CASE,
Case taking: Done by the whole sub-group
Presenter: Kyaw San Lin (RN - 21)
Computer: Kay Yu San (RN- 4)
KK Thwe Sunn (RN - 1)Kyaw San Lin (RN - 21)
Pamphlet: KK Thwe Sunn (RN - 1)

CONTENTS
Personal CharacteristicsSummary of Relevant Social & Community Aspect
Summary of Clinical AspectsAnalysis of the ProblemManagementSummary of the Case
PERSONAL CHARACTERISTICS Age 29 Sex Female Race and Religion Myanmar, Buddhist Education 4th Standard Marital status Married Number of children 2 Occupation Selling rice & pickled tea (La-phat) at Thein Phyu Night Bazaar
PERSONAL CHARACTERISTICS Date of Admission 24th August, 2014 Hospital Ward Unit 3, B Block, Central Woman Hospital
Father Name U Sein Win Occupation Manual Worker Education Read & Write
Mother Name Daw Shwe Mi Occupation Manual Worker Education Read & Write
SUMMARY OF RELEVANT SOCIAL & COMMUNITY ASPECTPersonal HistoryOccupational HistoryFamily HistoryAttitude towards her illnessSocial Environmental History
PERSONAL HISTORY
Well conscious and can respond to questions
Hobby - Watching TV, mainly moviesDoesn’t have any ambition

HER LIFE EVENTS
Childhood life at Zwe
Htaw village
Moved to Yangon
Life after Marriage
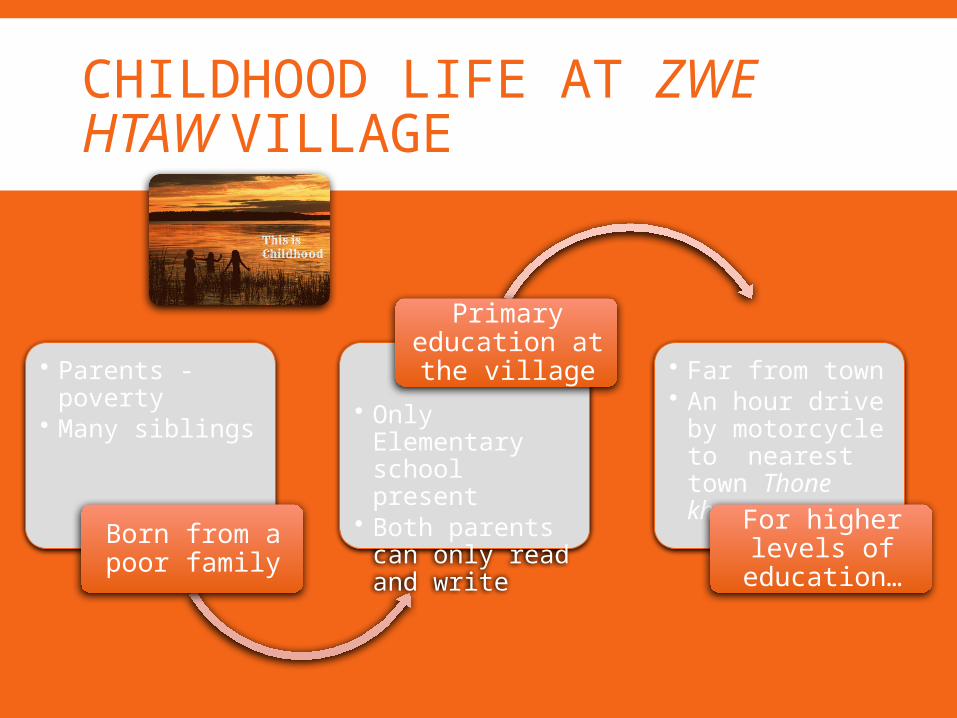
CHILDHOOD LIFE AT ZWE HTAW VILLAGE
• Parents - poverty
• Many siblings
Born from a poor family
• Only Elementary school present
• Both parents can only read and write
Primary education at the village • Far from town
• An hour drive by motorcycle to nearest town Thone khwa
For higher levels of
education…
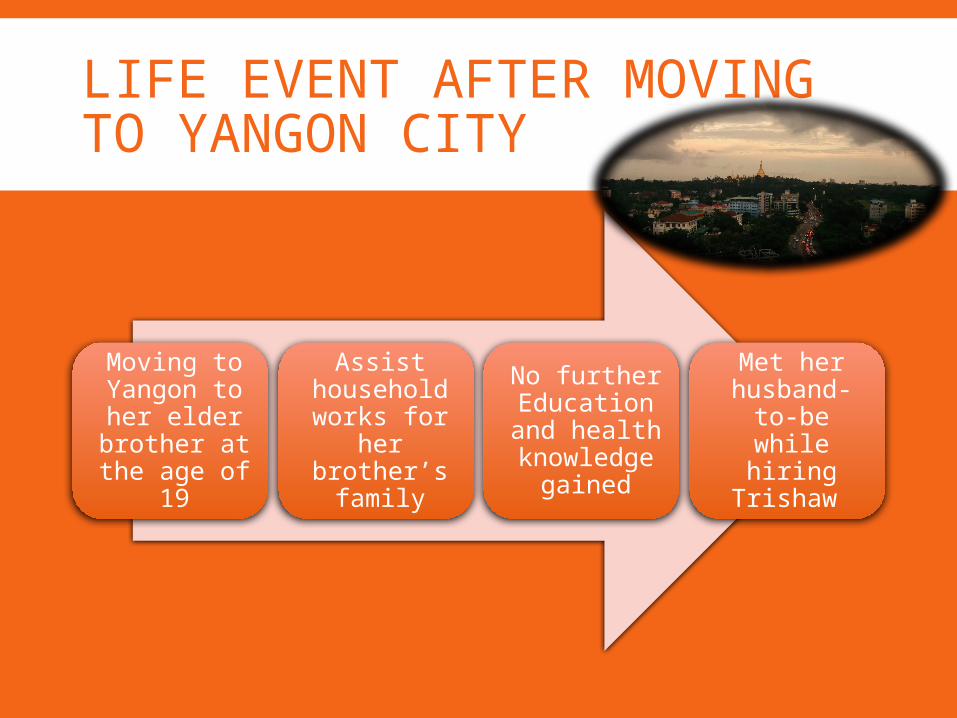
LIFE EVENT AFTER MOVING TO YANGON CITY
Moving to Yangon to her elder brother at the age of
19
Assist household works for
her brother’s
family
No further Education and health knowledge
gained
Met her husband-to-
be while hiring
Trishaw
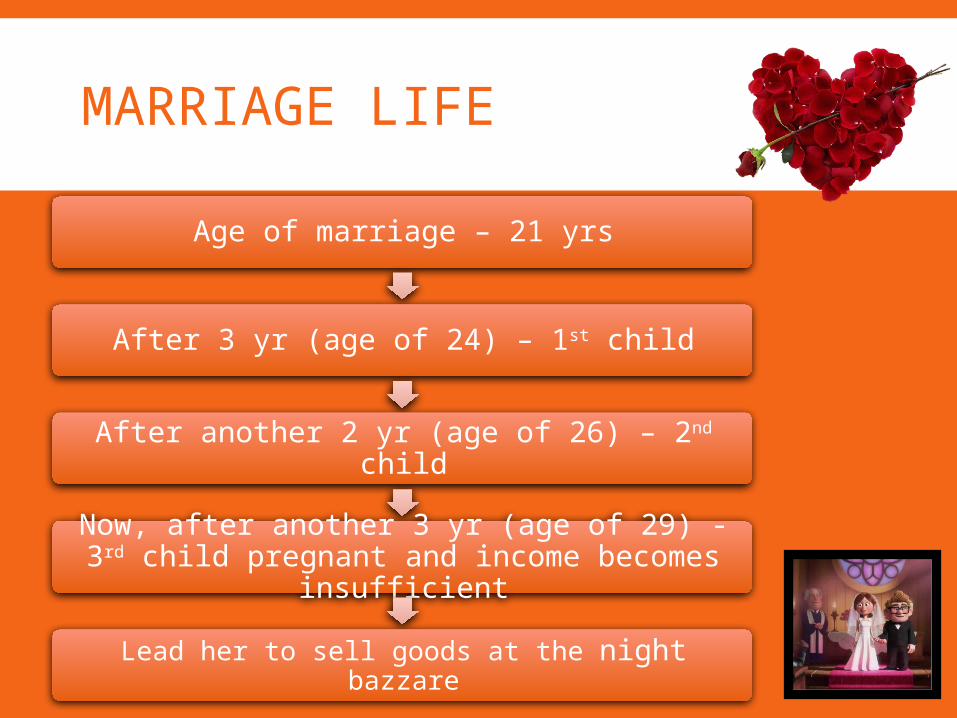
MARRIAGE LIFE
Age of marriage – 21 yrs
After 3 yr (age of 24) – 1st child
After another 2 yr (age of 26) – 2nd child
Now, after another 3 yr (age of 29) - 3rd child pregnant and income becomes insufficient
Lead her to sell goods at the night bazzare

OCCUPATIONAL HISTORY
Working hours
From 10 pm to 4 am
Abnormal sleeping pattern
Hours of sleep per day
4 hours
Insufficient hours of sleep
• Selling rice & pickled tea (La-phat) at Thein Phyu Night Bazaar
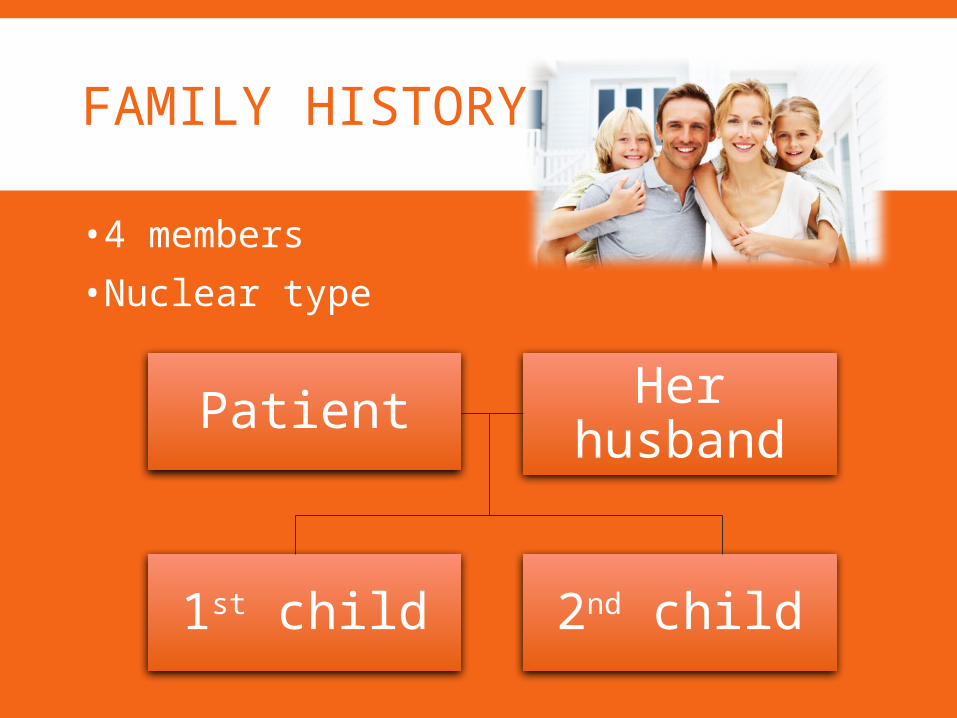
FAMILY HISTORY
•4 members•Nuclear type
Her husbandPatient
2nd child1st child
HER HUSBAND
Age – 33 yearsEducation – 4th StandardOccupation – trishaw driverDaily income – 5000 kyats

HER CHILDREN
First child - 5 years old, lives with her grandparents at Zwe Htaw village since 2012.
Second child – 3 ½ years old, sent to her grandparents since she have the present pregnancy
ATTITUDE TOWARDS HER ILLNESS According to her… She has never worked as sex worker No pre-marital sexual activity No extra-marital sexual activity Never transfused blood before
So,… Realised that she got this disease from her beloved husband.
Already known the chances of exposure to premarital and extramarital sexual exposure during his working period and environment.
ATTITUDE TOWARDS HER ILLNESSBut,… She understands her husband’s situation Still loves him… Wants to take medication regularly together with her husband.
To get be able to live with her family happily as normal people.
HER CURRENT ENVIRONMENT Lives only with her husband in a 10 square feet room Shared with other families. Share bathrooms and toilets.
Transportation - easy from her house. Bazaar - near her house and she can go easily. Water supply - from the Gyo Phyu water pipeline. Latrine - sanitary with septic tank attached. Refuse disposal - in a nearby public bin. Clinics and hospitals - situated near her house
SUMMARY OF CLINICAL ASPECT
HistoryPhysical Examination InvestigationsProvisional Diagnosis
HISTORY
Admitted to the Central Women Hospital (CWH)
On 24th August, 2014 For acute gastritis and PMCT programme
MENSTRUAL HISTORY
Age of menarche - 13 years. 28-week cycle, lasts for 3 days, regular, moderate amount, no dysmenorrhoea.
LMP - 3rd January, 2014 (not sure)MBD - 33 wks 6 days EDD - 10th October, 2014
PAST OBSTETRIC HISTORY
The age of marriage - 21 years. Single marriage. G 3, P 2+0.Her 1st child - 5 years old, born at term by urgent LSCS d/t APH d/t placenta praevia. No 3rd stage & puerperal complications.
Her 2nd child - 3 ½ years old, born at term by elective LSCS d/t previous LSCS. No 3rd stage & puerperal complications.
HISTORY OF PRESENT PREGNANCYUnplanned but wanted pregnancy. Dx of pregnancy by UCG on March. Signs and symptoms of pregnancy such as morning sickness, and amenorrhoea are also present.
Took AN care at 6th month of pregnancy at CWH.
HISTORY OF PRESENT ILLNESSacute onset dull aching pain in epigastrium 1 day duration aggravated by taking food relieved by taking antacidnot severeNo radiation
PAST MEDICAL & SURGICAL HISTORY
No past history of H/T, DM, IHD, epilepsy, TB, renal diseases or other diseases.
No history of hospitalization. No past surgical history.
PAST GYNAECOLOGICAL HISTORYNo past gynaecological diseases, operations or treatment.
Screening of cervical smear has not been done before.
FAMILY, DRUG & PERSONAL HISTORY
No family history of H/T, DM, PE, or twin pregnancy.
No other genetic diseases present.No regular taking of drug. No known drug allergy.No smoking, alcohol drinking, betel chewing or drugs addiction.
CLINICAL EXAMINATION
GeneralCNSCVSRespiration LymphaticsBreastAbdomen
GENERAL EXAMINATION Well alert, well orientated, lying comfortably in the bed, no fever, slightly thin.
Eyes: Pallor present. No Jaundice. Mouth: Teeth and gum are healthy. No tonsillar enlargement.
Neck: No visible swelling in the neck. Extremities
Upper limbs: NAD Lower limbs: No clubbing, no peripheral cyanosis, bilateral pitting petal oedema present.
CNS EXAMINATION
Well alert, well orientated. Normal cranial nerves, sensory, motor and peripheral nerves functioning.
CVS EXAMINATION
BP- 110/70 mmHgPR – 70 beats/min Apex beat - located at the left 5th ICS within the mid-clavicular line
Normal 1st and 2nd heart sound No added sound
RESPIRATORY SYSTEM EXAMINATIONNormal vesicular breath soundNo added soundRR – 16/min
LYMPHORETICULAR SYSTEM
No lymph node enlargement.No liver enlargement. No splenic enlargement.
BREAST EXAMINATION
Well developed. Nipple is protruded. On palpation of the four quadrants, no abnormal lump is palpated.
ABDOMINAL EXAMINATION (SUMMARY)Fundal Height - 38week sizeSFH- 35 cmSingle foetus Longitudinal lieHead presentationNot engaged.FHS is 160 beats/min, strong and regular.
INVESTIGATIONS Blood for CP – RBC, WBC, & platelet are normal in both count and morphology
Chemical Pathology – Alkaline Phosphatase↑ Infection screening HBs Ag - negative, HCV Ab - negative, Blood for VDRL – non-reactive
HIV screening test – reactive, 1st confirmation test – reactive, 2nd confirmation test – Positive
HIV screening test of the husband - reactive, 1st confirmation test – reactive, 2nd confirmation test – Positive
CD4 count - 284 cells/L (Normal - >400 cells/L)
INVESTIGATIONS
USGDate of present report 2nd July, 2014No. of foetus: SinglePresentation: Head Lie: LongitudinalPlacental Localization: Anterior, upperAmniotic fluid volume: NormalRadiologist Comments Single viable foetus 27 week at EGA
PROVISIONAL DIAGNOSIS
29 years oldG 3, P 2+0at 34+6 weeks of pregnancy with HIV infection and acute gastritis
ANALYSIS OF THE PROBLEM
From 3 Aspects:1. Social Etiology2. Diagnoses – Clinical & Social3. Social Implications
SOCIAL ETIOLOGY
Social Etiology
Predisposing Factors
Enabling Factors
Precipitating Factors
Reinforcing Factors
PREDISPOSING FACTORS
Poverty Husband’s daily income - 5 thousand kyats
Low Education Level passed only the 4th Standard
Poor Health Knowledge not interested in seeking health knowledge
Weak Guardianship d/t the large size of her family needs personality formation and moral teachings

ENABLING FACTORS
Low education Level of HusbandOccupation of HusbandMorality of Husband, Premarital Sexual Exposure,
Unsafe Sex Lack of Premarital Counselling
PRECIPITATING FACTORS
Pregnancy increases HIV infection progression, progression to AIDS and the chance of death.
Nature of her Occupation weakens her health and worsens her condition.

REINFORCING FACTORS
Poor Nutrition does not eat any meat other than small fish.
commonly eats vegetables → low protein diet.
Lack of Family Support Currently, only her husband staying with her
insufficient as family support.
CLINICAL DIAGNOSIS
29 years old, G 3, P 2+0, at 33+6 weeks of pregnancy with HIV infection and acute gastritis
SOCIAL DIAGNOSIS
PovertyPoor education Lack of health knowledge especially reproductive health
SOCIAL IMPLICATIONS
Social Implicatio
ns
Individual Level
Family Level
Community Level
National Level
INDIVIDUAL LEVEL
Psychological Stress others might ignore her socially isolated loss of support from family & friends emotional breakdown fear of opportunistic infections, anticipatory grief, shame, helplessness, and discrimination
FAMILY LEVEL
Increased risk of transmission of HIV from mother to child during pregnancy, birth or lactation
Financial problems Inability to work during pregnancy Increase in expenditure of healthcare and health facilities
Family Burden care given to her during gestation period → take effort and time of family members.
Reduction of care for other children

COMMUNITY LEVEL
Increased risk of transmission Increased workload for doctors and medico-social workers
NATIONAL LEVEL
Decreasing Human resources Increased incidence and prevalence of HIV infected person
Increased workload of health sector

Predisposing factors
Poverty Low Education Level Poor Health
Knowledge Weak Guardianship
Enabling Factors Low education Level
of Husband Occupation of
Husband Morality of Husband Premarital Sexual
Exposure, Unsafe Sex Lack of Premarital
Counselling Precipitating factor
Pregnancy Nature of Occupation
Reinforcing factors Poor Nutrition Lack of Family
Support
Clinical diagnosis
29 years old, G 3, P 2+0, at 33+6 weeks of pregnancy with HIV infection & acute gastritis
Social diagnosis
Poverty Poor education Lack of health
knowledge especially in reproductive health
Individual Level Psychological stress
Community Level Increased risk of
transmission Increased workload
for doctors and medico-social workers
Family Level• Increased risk of
transmission of HIV• Financial problems• Family Burden• Reduction of care for
other children
National Level Decreasing Human
resources Increased incidence
and prevalence of HIV infected person
Increased workload of health sector
Social Etiology
Social Implication
CLINICO-SOCIAL MANAGEMENTS
Mangements
Immediate Managem
ent
Individual Level
Family Level
Long-term Managem
ent
Individual Level
Family Level
Community Level
National Level

IMMEDIATE MANAGEMENTS
Individual LevelPsychological support and counsellingPMCTNutritionTreatment for acute gastritis
Family LevelCounsellingSterilizationARV Prophylaxis to Baby
LONG-TERM MANAGEMENTS
Individual LevelSocial support and ART treatmentRestSafe water and FoodAvoid handling petsSafe Sex
Family LevelHealth EducationPrevention of HIV transmission

COMMUNITY LEVEL
HE about blood transfusion, drug abuse, sexual promiscuity and their disease
HE to sex workers about safe sex Encouraging the community to help patients by giving psychological support
Cooperation and collaboration with social welfare services such as NGOs
NATIONAL LEVEL Promoting literacy Creating job opportunities Promoting national health care services and facilities
National HIV/ AIDS Control Program (NAP) Implementing PMCT programme Surveillance against STD in community Identify missing cases Cooperation and collaboration with INGOs, local NGOs and services
Supervision, monitoring and evaluation
SUMMARY OF THE CASE
A female patient, aged 29, G 3, P 2+0, came to CWH for acute gastritis and AN Care.
HIV testing done as part of the AN Care package - positive result
Admitted to CWH, B Block, Unit 3 on 24th August, 2014 for PMCT.
Her husband tested for HIV - positive. Both - low income, poor educational status and lack of reproductive health education.
SUMMARY OF THE CASE
CD4 count - <350 cells/mm ART treatment Her husband - referred to Tharketa STI Hospital for ART treatment.
Counselling - HIV, PMCT, delivery and infant feeding

THANK YOU
FOR YOUR ATTENTION!!!
ANY QUESTION???