Avances en el tratamiento del estado epil+®ptico en el paciente cr+¡tico (2007)
24
Advances in the Management of Seizures and Status Epilepticus in Critically Ill Patients Karine J. Abou Khaled, MD, Lawrence J. Hirsch, MD * Comprehensive Epilepsy Center, Department of Neurology, Columbia University Neurological Institute, 7th floor, 710 West 168th Street, New York, NY 10032, USA Seizures and status epilepticus (SE) in the intensive care setting can be seen in two main groups of patients: patients admitted to the ICU because of continuous or repetitive seizures requiring aggressive treatment and pa- tients admitted for medical or surgical reasons who develop seizures during the course of their ICU stay. This article discusses new concepts of seizures and SE in the adult ICU, including nonconvulsive seizures. First, SE epide- miology, definition, classification, etiologies, diagnosis, and prognosis are briefly reviewed. Systemic and neurologic e ff ects of seizures and SE are dis- cussed. Finally, the authors propose strategic therapeutic steps and focus on the treatment of seizures and SE in patients with specific organ failures or after organ transplantation. Epidemiology and definition SE remains a serious, life-threatening emergency. De Lorenzo and col- leagues [1] estimated that it aff ects 152,000 individuals in the United States per year and causes 42,000 deaths. The first attempt to define SE was in 1962, when the tenth European conference on epileptology and clinical neu- rophysiology defined SE as ‘‘ a condit ion characteriz ed by an epil epti c seizure which is so frequently repeated or so prolonged as to create a fixed and lasting epileptic condition’’ [2]. The International Classification of Ep- ileptic Seizures, along with a general consensus, described SE as any seizure lasting more than 30 minutes or intermittent seizures from which the patient did not regain consciousness lasting for more than 30 minutes [2]. The ratio- nale for choosing 30 minutes was based on the minimum duration thought * Corresponding author. E-mail address: [email protected] (L.J. Hirsch). 0749-0704/07/$ - see front matter Ó 2007 Elsevier Inc. All rights reserved. Crit Care Clin 22 (2007) 637–659
-
Upload
azucena-zapata-rivera -
Category
Documents
-
view
225 -
download
0
Transcript of Avances en el tratamiento del estado epil+®ptico en el paciente cr+¡tico (2007)
8/8/2019 Avances en el tratamiento del estado epil+®ptico en el paciente cr+¡tico (2007)
http://slidepdf.com/reader/full/avances-en-el-tratamiento-del-estado-epilptico-en-el-paciente-crtico 1/23
Advances in the Management
of Seizures and Status Epilepticus
in Critically Ill Patients
Karine J. Abou Khaled, MD, Lawrence J. Hirsch, MD*
Comprehensive Epilepsy Center, Department of Neurology, Columbia University
Neurological Institute, 7th floor, 710 West 168th Street, New York, NY 10032, USA
Seizures and status epilepticus (SE) in the intensive care setting can be
seen in two main groups of patients: patients admitted to the ICU because
of continuous or repetitive seizures requiring aggressive treatment and pa-
tients admitted for medical or surgical reasons who develop seizures during
the course of their ICU stay. This article discusses new concepts of seizures
and SE in the adult ICU, including nonconvulsive seizures. First, SE epide-
miology, definition, classification, etiologies, diagnosis, and prognosis are
briefly reviewed. Systemic and neurologic eff ects of seizures and SE are dis-
cussed. Finally, the authors propose strategic therapeutic steps and focus on
the treatment of seizures and SE in patients with specific organ failures or
after organ transplantation.
Epidemiology and definition
SE remains a serious, life-threatening emergency. De Lorenzo and col-leagues [1] estimated that it aff ects 152,000 individuals in the United States
per year and causes 42,000 deaths. The first attempt to define SE was in
1962, when the tenth European conference on epileptology and clinical neu-
rophysiology defined SE as ‘‘a condition characterized by an epileptic
seizure which is so frequently repeated or so prolonged as to create a fixed
and lasting epileptic condition’’ [2]. The International Classification of Ep-
ileptic Seizures, along with a general consensus, described SE as any seizure
lasting more than 30 minutes or intermittent seizures from which the patient
did not regain consciousness lasting for more than 30 minutes [2]. The ratio-nale for choosing 30 minutes was based on the minimum duration thought
* Corresponding author.
E-mail address: [email protected] (L.J. Hirsch).
0749-0704/07/$ - see front matter Ó 2007 Elsevier Inc. All rights reserved.
doi:10.1016/j.ccc.2006.06.004 criticalcare.theclinics.com
Crit Care Clin 22 (2007) 637–659
8/8/2019 Avances en el tratamiento del estado epil+®ptico en el paciente cr+¡tico (2007)
http://slidepdf.com/reader/full/avances-en-el-tratamiento-del-estado-epilptico-en-el-paciente-crtico 2/23
to result in neuronal injury in animal models. Bleck [3] defined SE as con-
tinuous or repeated seizures lasting more than 20 minutes. More recently,
Lowenstein and colleagues [4] suggested that defining SE based on the the-oretical onset of neuronal injury is of questionable value because of the com-
plexity of this relation in humans. They suggested that ‘‘we should not wait
10 minutes or longer before instituting a treatment protocol for SE’’ [4].
Treiman and coworkers [5] defined overt convulsive SE as two or more
generalized convulsions without full recovery of consciousness between
seizures, or continuous convulsive activity for more than 10 minutes. For
practical purposes, SE should be considered if a seizure persists more
than 5 minutes because very few single seizures last this long.
Classification of status epilepticus
In 1967, Gastaut [2] first distinguished two major types of SE based
exclusively on seizure semiology. The first type is generalized SE, which is
subdivided into two groups:
1. Generalized convulsive SE (GCSE) (tonic-clonic SE or grand mal SE,
tonic SE, clonic SE, myoclonic SE)
2. Nonconvulsive generalized SE, including petit mal status
The second type is partial SE, which is subdivided into two groups:
1. Simple partial SE (eg, somatomotor or aphasic SE)
2. Complex partial SE
Gastaut separately distinguished a unilateral SE, seen only in infants and
very young children, and erratic SE, seen in neonates.
There is no recent consensus on further classification of nonconvulsive
status epilepticus (NCSE). In clinical practice, it often is impossible to dif-
ferentiate between NCSE of generalized onset and NCSE of partial onsetwith bilateral spread. The authors divide SE into convulsive SE and
NCSE or subtle SE. The authors reserve the term absence SE for patients
with chronic primary or symptomatic generalized epilepsy. There are two
distinct clinical scenarios involving NCSE: that in ambulatory patients
with confusion who have a good prognosis and often respond quickly and
dramatically to treatment in the emergency department, and that in coma-
tose/stuporous patients who have a more guarded prognosis and rarely
awaken rapidly with treatment. The latter situation is discussed further in
this article.
Etiologies
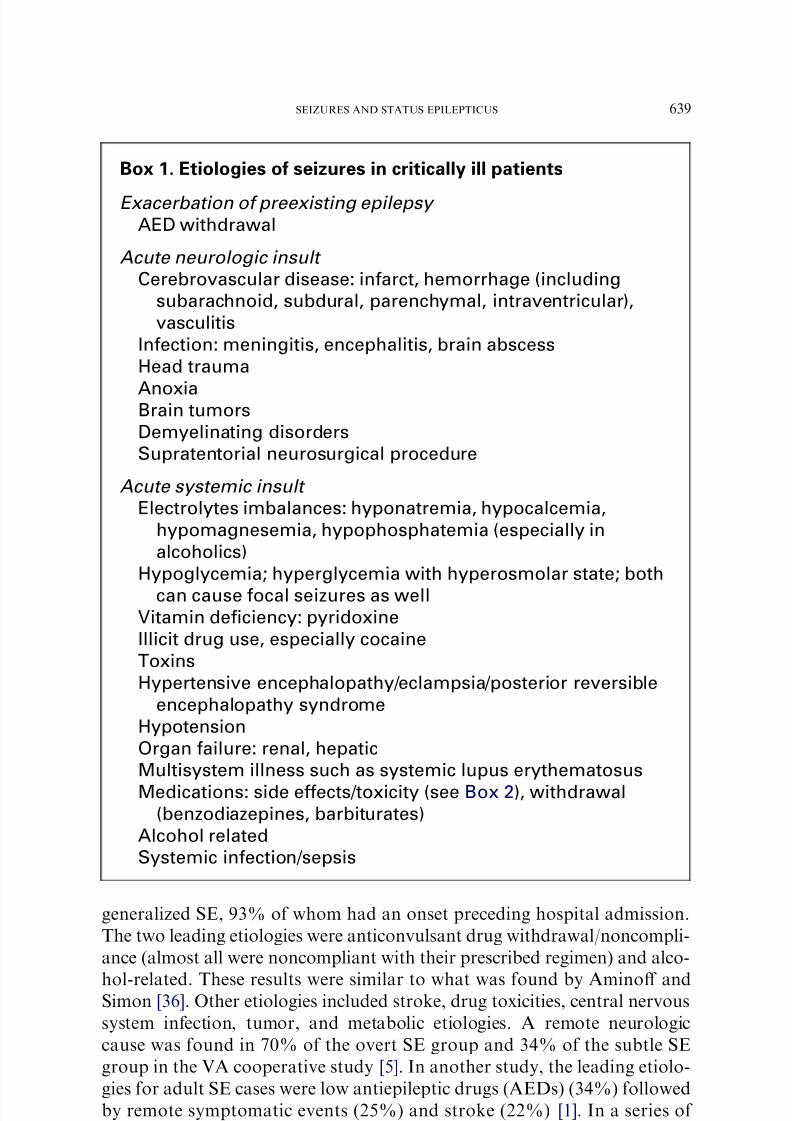
Seizures in the ICU can arise from various etiologies. Etiologies diff er
among centers, patient population, and age. Box 1 summarizes these by cat-
egories. Lowenstein and Alldredge [6] evaluated 154 patients treated for
638 ABOU KHALED & HIRSCH
8/8/2019 Avances en el tratamiento del estado epil+®ptico en el paciente cr+¡tico (2007)
http://slidepdf.com/reader/full/avances-en-el-tratamiento-del-estado-epilptico-en-el-paciente-crtico 3/23
generalized SE, 93% of whom had an onset preceding hospital admission.
The two leading etiologies were anticonvulsant drug withdrawal/noncompli-
ance (almost all were noncompliant with their prescribed regimen) and alco-
hol-related. These results were similar to what was found by Aminoff andSimon [36]. Other etiologies included stroke, drug toxicities, central nervous
system infection, tumor, and metabolic etiologies. A remote neurologic
cause was found in 70% of the overt SE group and 34% of the subtle SE
group in the VA cooperative study [5]. In another study, the leading etiolo-
gies for adult SE cases were low antiepileptic drugs (AEDs) (34%) followed
by remote symptomatic events (25%) and stroke (22%) [1]. In a series of
Box 1. Etiologies of seizures in critically ill patients
Exacerbation of preexisting epilepsy AED withdrawal
Acute neurologic insult
Cerebrovascular disease: infarct, hemorrhage (including
subarachnoid, subdural, parenchymal, intraventricular),
vasculitis
Infection: meningitis, encephalitis, brain abscess
Head trauma
AnoxiaBrain tumors
Demyelinating disorders
Supratentorial neurosurgical procedure
Acute systemic insult
Electrolytes imbalances: hyponatremia, hypocalcemia,
hypomagnesemia, hypophosphatemia (especially in
alcoholics)
Hypoglycemia; hyperglycemia with hyperosmolar state; both
can cause focal seizures as wellVitamin deficiency: pyridoxine
Illicit drug use, especially cocaine
Toxins
Hypertensive encephalopathy/eclampsia/posterior reversible
encephalopathy syndrome
Hypotension
Organ failure: renal, hepatic
Multisystem illness such as systemic lupus erythematosus
Medications: side effects/toxicity (see Box 2), withdrawal(benzodiazepines, barbiturates)
Alcohol related
Systemic infection/sepsis
639SEIZURES AND STATUS EPILEPTICUS

8/8/2019 Avances en el tratamiento del estado epil+®ptico en el paciente cr+¡tico (2007)
http://slidepdf.com/reader/full/avances-en-el-tratamiento-del-estado-epilptico-en-el-paciente-crtico 4/23
patients with NCSE, Towne and associates [7] identified hypoxia/anoxia as the
most frequent etiology (42%) followed by cerebrovascular accident (22%).
Treatment of the underlying cause may be crucial to managing seizures
successfully, especially when due to a toxic/metabolic origin. It is often dif-
ficult, however, to identify a single etiology because of the presence of mul-
tiple factors lowering the seizure threshold, including the acute medical or
neurologic process, medications, renal or hepatic failure, infection, fever,
hypoxia, metabolic abnormalities, or alkalosis. Because of this complexity,
it is difficult to define the incidence of drug-induced seizures in ICU patients.
Imipenem commonly is cited for its association with seizures. One study
found that imipenem use was associated with an increased risk for seizures,
but most of these occurred when the patient was not taking imipenem [8].
This finding highlighted the possibility that imipenem was a confounding
variable, a marker of severity of illness and infection, rather than a contrib-
utor to the seizures. Box 2 lists the major categories of medications that have
been incriminated in contributing to seizures.
Diagnosis
NCSE is underdiagnosed. It can present in many ways, including
mild personality changes, lethargy, agitation, blinking, confusion, facial
Box 2. Medications associated with decreased seizure threshold
Antidepressants, mostly bupropion and maprotilineNeuroleptics, mostly phenothiazines and clozapine
Lithium
Baclofen
Withdrawal of AEDs
Phenytoin at supratherapeutic levels (including very high free
levels)
Theophylline
Analgesics: meperidine, fentanyl, and tramadol
Opioid withdrawalBenzodiazepine withdrawal
Barbiturate withdrawal
Antibiotics: b-lactams (cefazolin), carbapenems (imipenem),
quinolones, isoniazid (treat with vitamin B6), metronidazole
Antiarrhythmic medications: mexiletine, lidocaine, digoxin
Radiographic contrast agents
Immunomodulators: cyclosporine, tacrolimus, interferons
Chemotherapeutic agents: alkylating agents such as
chlorambucil and busulfan
Data from refs. [91–93].
640 ABOU KHALED & HIRSCH

8/8/2019 Avances en el tratamiento del estado epil+®ptico en el paciente cr+¡tico (2007)
http://slidepdf.com/reader/full/avances-en-el-tratamiento-del-estado-epilptico-en-el-paciente-crtico 5/23
twitching, automatisms, and coma [9,10]. Nonconvulsive seizures may con-
tinue even after clinical seizures have ceased. In the Richmond study, 14%
of patients who stopped seizing clinically showed persistent electrographicSE on electroencephalogram (EEG), and 48% had intermittent electro-
graphic seizures [11]. Nonconvulsive seizures have been reported in 34%
of neurologic ICU patients [12], 16% of severe head trauma patients [13],
and 8% of comatose patients who had no prior seizures or subtle clinical
evidence of seizures [7]. In the authors’ series of 570 consecutive inpatients
undergoing continuous EEG monitoring at Columbia, 110 (19%) had sei-
zures, and 101 of these 110 patients (92%) had purely nonconvulsive sei-
zures that could be detected only by EEG. Only half of these patients had
their first seizure within the first hour of recording; even a prolonged routineEEG would not have identified the nonconvulsive seizures in half the
patients. The authors concluded that 24 hours was a reasonable screen for
nonconvulsive seizures in noncomatose patients (95% of noncomatose
patients had their first seizure by 24 hours), but that 48 hours or more
may be needed in comatose patients (only 80% had their first seizure by
24 hours) [14].
Prognosis
The overall mortality after SE is similar in the two largest known US
studies: 21% in Rochester, Minnesota [15], and 22% in Richmond, Virginia
[16] (but higher in the elderly population, 38% [17]).Towne and colleagues
[18] reported 1-month outcome of 253 adult patients with SE and showed
that the mortality rate of patients with prolonged SE (O60 minutes) was
32% compared with 2.7% in patients whose SE was 30 to 59 minutes. Mor-
tality was increased in patients older than 70 years of age. Conflicting data
exist regarding mortality and morbidity of NCSE, depending primarily on
patient selection. The highest reported mortality rates have been 52%[7,19]. Shneker and Fountain [20] found that 18% of patients with NCSE
died. Patients in the acute medical group (defined as acute neurologic or sys-
temic problems or both) had significantly higher mortality rates (27%) than
patients in the cryptogenic (18%) or epilepsy (3%) group. Worse outcome
also was associated with severely impaired mental status.
Sequelae of status epilepticus
Cerebral changes
Lothman and colleagues [21] developed and characterized the self-sus-
taining limbic SE electrogenic animal model using continuous hippocampal
stimulation. As SE progresses, the animals show fewer motor manifestations
despite ongoing electrographic seizure activity. Self-sustaining limbic SE
stops spontaneously after several hours, and the animals gradually recover
641SEIZURES AND STATUS EPILEPTICUS
8/8/2019 Avances en el tratamiento del estado epil+®ptico en el paciente cr+¡tico (2007)
http://slidepdf.com/reader/full/avances-en-el-tratamiento-del-estado-epilptico-en-el-paciente-crtico 6/23
to normal alertness. Approximately 9 months later, they begin to have spon-
taneous recurrent partial seizures that persist for more than 1 year. This
model shows that acute SE can lead to long-term epilepsy.Recurrent spontaneous seizures are frequent sequelae of GCSE and are
present after induced SE in several animal models. What about sequelae
of recurrent seizures in humans? New markers, such as serum neuron-spe-
cific enolase (a glycolytic enzyme found primarily within neurons), are being
investigated as markers of neuronal injury. In the animal literature, neuron-
specific enolase correlates with the amount of histologic injury in rats after
lithium-pilocarpine–induced SE [22]. Elevated levels of serum neuron-spe-
cific enolase have been documented in patients after nonconvulsive SE, in-
cluding in cases without any radiographically demonstrable acute braininjury [23–26]. The subtype of SE that was associated with the highest serum
neuron-specific enolase levels was subclinical SE in critically ill patients [24].
These acute seizure-related changes also can be shown by diff erent mag-
netic resonance neuroimaging modalities. There are several reported cases of
SE with clear development of acute hippocampal swelling on MRI followed
by later hippocampal atrophy and abnormal signal, evidence of mesial tem-
poral sclerosis [27–29]. Pathologic and histologic changes also have been
shown. DeGiorgio and colleagues [30] used a case-control approach and
cell-density quantification to analyze changes in the hippocampus of fivepatients who died after GCSE. They found significant pyramidal cell loss
in these patients compared with a control group. Changes attributable
directly to the occurrence of GCSE are difficult to determine because path-
ologic alterations could have been present as a result of prior history of re-
petitive seizures or other acute processes. Chronic sequelae result from cell
loss or altered physiology or synaptic connectivity. Focal or diff use cortical
damage has been described. The latter accounts for general cognitive
changes, whereas hippocampal neuronal loss can explain the subsequent
deficits in memory that are sometimes seen [31].
Changes in systemic physiology
The first 30 minutes of GCSE are dominated by sympathetic overdrive,
probably mediated by increased circulating catecholamines, following which
physiologic changes begin to normalize or move in the opposite direction, as
a result of failure of homeostatic mechanisms [32]. The most important phys-
iologic perturbations are fever, blood pressure changes, cardiac arrhythmias,
pulmonary vascular pressure changes, and alterations in blood chemistries.
Fever is common secondary to sustained muscle activity. Clinicians
should be cautious in ruling out infection before attributing fever to
SE, especially if associated with increased white blood cells in blood
or cerebrospinal fluid. Meldrum and coworkers [33] found that in-
creased temperature correlated with severity of cerebral injury and
found that neuromuscular blockade prevented both.
642 ABOU KHALED & HIRSCH
8/8/2019 Avances en el tratamiento del estado epil+®ptico en el paciente cr+¡tico (2007)
http://slidepdf.com/reader/full/avances-en-el-tratamiento-del-estado-epilptico-en-el-paciente-crtico 7/23
Systemic blood pressure increases early in SE, but tends to fall to normal
or below normal later in GCSE.
Cardiac arrhythmias can be life-threatening in SE. Boggs and associates[34] reported specific electrocardiogram (ECG) abnormalities not pres-
ent at baseline, including in 58.3% of patients in SE. The most fre-
quently observed abnormalities were ischemic changes. They also found
that patients with ECG abnormalities had a higher mortality (37%
versus 12% in patients without ECG changes). Excessive endogenous
epinephrine release has been implicated in cardiac contraction band
necrosis. Manno and colleagues [35] reviewed the cardiac pathologic
slides of 11 patients who died during an episode of SE and found
contraction band necrosis in 8 of them compared with 5 of 22 controlpatients (P ! .05).
Pulmonary arterial pressures increase in SE, and pulmonary edema
might occur in the setting of sympathetic hyperactivity [32].
Blood chemistry changes observed in SE include the following:
Severe metabolic acidosis may be seen secondary to excess anaerobic
metabolic activity.
Hyperkalemia may be seen secondary to acidosis and muscle necrosis.
Hyperglycemia resulting from increased catecholamines, but with pro-
longed SE increased insulin secretion may result in hypoglycemia, Increased creatine kinase levels resulting from rhabdomyolysis can be
seen after prolonged convulsions and might lead to acute renal failure.
Increased prolactin level 10 to 20 minutes after a suspected event has
been documented to be useful in diff erentiating epileptic from nonepi-
leptic convulsions, but there is no evidence of the level being useful in
SE [36].
Leukocytosis from demargination but should not be attributed to SE,
unless infectious etiologies are ruled out.
In a series of 138 patients who had cerebrospinal fluid analysis duringSE, Barry and Hauser [37] found that 22.5% had abnormal cerebrospi-
nal fluid white blood cell count or diff erential. The highest white blood
cell count in patients with no acute insult was 28 Â 106/L. A mild tran-
sient increase in protein content also may be observed, possibly reflect-
ing breakdown of the blood-brain barrier [38].
Treatment of acute seizures and status epilepticus
Management of SE should begin within 5 minutes of seizure activity orafter two seizures without full recovery in between. In the setting of acute
brain injury, treatment usually should be initiated after a single self-limited
seizure, at least for the short-term, and especially in patients with increased
intracranial pressure or patients in whom an episode of marked hyperten-
sion and tachycardia would be dangerous. General supportive measures
for seizures and SE are reviewed first. Subsequently, specific treatments
643SEIZURES AND STATUS EPILEPTICUS

8/8/2019 Avances en el tratamiento del estado epil+®ptico en el paciente cr+¡tico (2007)
http://slidepdf.com/reader/full/avances-en-el-tratamiento-del-estado-epilptico-en-el-paciente-crtico 8/23
and choice of AEDs are reviewed. Treatment in special situations, including
organ failure and immunosuppression, conditions commonly encountered
in the ICU, also is addressed.
General supportive measures
General supportive measures begin with basic life support measures and
adequate monitoring of vital signs and ECG. A proposed timetable and
treatment protocol is represented in Table 1.
Blood pressure should be monitored closely, especially if seizures persist for
more than 30 minutes, at which point cerebral autoregulation starts to fail,
and cerebral perfusion becomes increasingly dependent on systemic blood
pressure. At this point, intravenous drugs, such as propofol, benzodiazepines,
and phenobarbital, frequently are introduced, and intravenous fluid resuscita-
tion and vasopressors may become necessary. Refractory GCSE and the use of
agents such as midazolam, propofol, and pentobarbital generally mandate se-
curing the airway and instituting mechanical ventilation.
The treatment should aim to correct all underlying potential causes and
stop the seizures simultaneously. In at least half of cases of SE, there is some
acute etiology that warrants attention. Depending on the clinical presenta-
tion, additional tests might be necessary when the patient is stabilized, in-
cluding lumbar puncture and head CT or MRI, to rule out acute
structural or potentially treatable etiologies.
Pharmacologic therapy
Early initiation of therapeutic intervention is much more important than
the choice of agent used. Mazarati and colleagues [39] showed in animal ex-
periments that the efficacy of phenytoin decreased dramatically with time,
and proposed that the failure of diazepam and phenytoin to abort self-sus-
taining SE during its maintenance phase implies that ‘‘seizures evolve certainmechanisms that cause refractoriness to antiepileptic drugs.’’ Although phe-
nytoin and benzodiazepines become less eff ective, glutamate antagonists,
such as ketamine (an N -methyl-D-aspartate [NMDA] antagonist), are inef-
fective initially, but become eff ective in later stages in animals. In humans,
intervention within the first 30 minutes of seizure onset was associated
with 80% response to first-line drugs. The response rate declined with longer
intervals such that more than 60% of the patients who were in SE for more
than 2 hours before initiation of treatment failed to respond to the first-line
treatment [6]. AEDs should be selected in consideration of the patients’prior history, medications, allergies, hemodynamic status, and hepatic and
renal function and the physician’s experience and preference.
Only a few randomized controlled trials have compared treatment strat-
egies in SE. The most important one was the VA Status Epilepticus Coop-
erative Study [5], which compared the efficacy of four drugs for the
treatment of GCSE. A total of 518 patients were randomly assigned to
644 ABOU KHALED & HIRSCH

8/8/2019 Avances en el tratamiento del estado epil+®ptico en el paciente cr+¡tico (2007)
http://slidepdf.com/reader/full/avances-en-el-tratamiento-del-estado-epilptico-en-el-paciente-crtico 9/23
receive phenobarbital (15 mg/kg), phenytoin (18 mg/kg), diazepam (0.15
mg/kg) plus phenytoin (18 mg/kg), or lorazepam (0.1 mg/kg). The first reg-
imen chosen was successful in 55.5% of patients with ‘‘overt status,’’ but
only 14.9% of patients with ‘‘subtle SE’’ (coma and ictal discharges on
Table 1
Status epilepticus d adult treatment protocola
Time min Action0–5 Diagnose; give O2; ABCs; obtain IV access; begin ECG monitoring; draw blood
for Chem-7, magnesium, calcium, phosphate, CBC, LFTs, AED levels, ABG,
troponin; toxicology screen (urine and blood)
6–10 Thiamine 100 mg IV; 50 mL of D50 IV unless adequate glucose known.
Lorazepam 4 mg IV over 2 min; if still seizing, repeat X 1 in 5 min. If no rapid IV
access, give diazepam 20 mg PR or midazolam 10 mg intranasally, buccally
or IMb.
10–20 If seizures persist, begin fosphenytoin 20 mg/kg IV at 150 mg/min, with blood
pressure and ECG monitoring. This step can be skipped initially, especially if
proceeding to midazolam or propofol, or can be performed simultaneously with
the next step; if done simultaneously, administration rate can be slowed
10–60 If seizures persist, give one of the following (intubation necessary except for
valproate):
CIV midazolam: Load: 0.2 mg/kg; repeat 0.2–0.4 mg/kg boluses every 5 min until
seizures stop, up to a maximum total loading dose of 2 mg/kg. Initial CIV rate:
0.1 mg/kg/h. CIV dose range: 0.05–2.9 mg/kg/h, titrate to EEG seizure control
or burst suppression. If still seizing, add or switch to propofol or pentobarbital.
or
CIV propofol: Load: 1–2 mg/kg; repeat 1–2 mg/kg boluses every 3–5 min until
seizures stop, up to maximum total loading dose of 10 mg/kg. Initial CIV rate:
2 mg/kg/h. CIV dose range: 1–15 mg/kg/h, titrate to EEG seizure control or
burst suppression. If still seizing, add or switch to midazolam or pentobarbital.
Avoid using O5 mg/kg/h for multiple days to minimize risk of propofol
infusion syndrome. Follow CPK, triglycerides, acid-base status closely.
or
IV valproate: 30–40 mg/kg over w10 min. If still seizing, additional 20 mg/kg
over w5 min. If still seizing, add or switch to CIV midazolam or propofol.
or
IV phenobarbital: 20 mg/kg IV at 50–100 mg/min. If still seizing, add or switch to
CIV midazolam, propofol, or pentobarbital.
O60 CIV pentobarbital. Load: 5 mg/kg up to 50 mg/min; repeat 5 mg/kg boluses until
seizures stop. Initial CIV rate: 1 mg/kg/h. CIV-dose range: 0.5–10 mg/kg/h;traditionally titrated to suppression-burst on EEG, but titrating to seizure
suppression is reasonable as well
Begin EEG monitoring ASAP if patient does not rapidly awaken or if any CIV
treatment is used.
Abbreviations: CIV, continuous intravenous; ABCs, stabilize airway, breathing and circula-
tion; ASAP, as soon as possible.a Columbia University Comprehensive Epilepsy Center, 2006.b The IV solution of diazepam can be given rectally if Diastat is not available; the IV solu-
tion of midazolam can be given by any of these routes.
Courtesy of the Columbia University Comprehensive Epilepsy Center, New York, NY.
645SEIZURES AND STATUS EPILEPTICUS
8/8/2019 Avances en el tratamiento del estado epil+®ptico en el paciente cr+¡tico (2007)
http://slidepdf.com/reader/full/avances-en-el-tratamiento-del-estado-epilptico-en-el-paciente-crtico 10/23
EEG with or without subtle movements). In patients with ‘‘overt status,’’ in-
travenous lorazepam was most eff ective. It stopped SE in 65% of the cases;
phenobarbital, 58%; diazepam plus phenytoin, 56%; and phenytoin alone,44%. The only statistically significant diff erences were between phenytoin
alone and lorazepam. Hypotension requiring treatment occurred more often
in patients with subtle SE, but there were no diff erences between the medi-
cations. Overall mortality was twice as high for patients whose SE was not
controlled with the first drug as for patients who had successful response to
the first regimen. In the VA cooperative study, patients who failed the first
treatment rarely responded to the second (7%) or third (2.3%), raising the
question of the efficacy of a second and third drug [5,40].
Lorazepam has many advantages over other drugs. It can be givenquickly and has a duration of antiseizure eff ect of 12 to 24 hours [41]. Lep-
pik and colleagues [41] compared lorazepam with diazepam for the treat-
ment of SE in 78 patients enrolled in a double-blind, randomized trial.
Time of onset of the two drugs was almost the same. Seizures were con-
trolled in 89% of the episodes treated with lorazepam and in 76% treated
with diazepam. These results, combined with the more recent and more de-
finitive VA cooperative study, have led to intravenous lorazepam (0.1 mg/kg)
becoming a clear drug of choice for initial treatment of SE.
No randomized controlled studies have been conducted for second-linetherapy, but phenytoin or fosphenytoin is the most frequently recommended
agent [9,42]. A loading dose of 18 to 20 mg/kg intravenously is recommen-
ded. Phenytoin solution is highly caustic to veins and may cause tissue ne-
crosis in case of extravasation, limiting the rate of administration to
a maximum of 50 mg/min. Fast administration carries the risk of hypoten-
sion and cardiac arrhythmias and requires close monitoring of blood pres-
sure and ECG. Fosphenytoin sodium is a phenytoin prodrug, preferred
over phenytoin because of its water solubility, allowing faster administra-
tion with less risk of venous irritation. It is rapidly dephosphorylated inthe bloodstream to phenytoin, with a half-life of 10 to 15 minutes, reaching
therapeutic free phenytoin levels slightly faster than intravenous phenytoin.
Cardiac complications and hypotension still can occur with fosphenytoin
(owing to the phenytoin).
Free phenytoin levels should be monitored with a goal of 1.5 to 2.5 mg/
mL, which is equivalent to a total phenytoin level of 15 to 25 mg/mL in
the presence of normal protein binding [9]. Free levels may be excessively
high in the presence of low albumin or coadministration of highly protein
bound drugs (eg, valproic acid [VPA]), and this may confuse the clinical pre-sentation by worsening encephalopathy or paradoxically exacerbating sei-
zures. Another common problem in ICU patients who are receiving
parenteral nutrition is decreased enteral phenytoin absorption and blood
levels after conversion of intravenous phenytoin to oral phenytoin with sub-
sequent poor seizure control. In a study by Bauer [43], phenytoin serum
levels decreased an average of 71.6% when parenteral nutrition was given
646 ABOU KHALED & HIRSCH

8/8/2019 Avances en el tratamiento del estado epil+®ptico en el paciente cr+¡tico (2007)
http://slidepdf.com/reader/full/avances-en-el-tratamiento-del-estado-epilptico-en-el-paciente-crtico 11/23
concurrently. This problem may be overcome if parenteral nutrition is with-
held temporarily before and after administration of oral phenytoin to these
patients.An alternative as second-line therapy is phenobarbital with a loading
dose of 15 to 20 mg/kg. Maximum rate is 50 to 100 mg/min. Recommended
serum levels in SE are greater than 30 mg/mL. It has a prolonged half-life in
adults ranging from 50 to 150 hours and is a powerful sedative that may
contribute to coma and mask the evolution of the neurologic examination
in critically ill patients. In addition, phenobarbital may cause respiratory de-
pression and hypotension via vasodilation and cardiac depression. The main
advantages are intravenous availability, prolonged eff ect, and good efficacy
in controlling SE.Interest in VPA for the treatment of SE has increased with the availability
of an intravenous formulation. It is highly bound to plasma protein, similar to
phenytoin, with similar caveats about its use. It diff ers from older generation
AEDs in being an enzyme inhibitor, rather than inducer; one must be vigilant
for increased levels or eff ect of concomitant P-450-metabolized medications.
There is a dramatic fall of its level after addition of antibiotics such as mero-
penem or amikacin, possibly owing to accelerated renal excretion [44].
Valproate has broad-spectrum activity against all types of seizures, in-
cluding postanoxic myoclonus. A major advantage is not causing sedationor hypotension, which renders it a drug of choice in patients with a ‘‘do
not intubate’’ status or phenytoin allergy (although it has not been approved
for use in SE). Intravenous VPA has been used in open-label studies with
approximately 80% seizure control [45,46]. Giroud and colleagues [46]
found that intravenous VPA stopped SE in 19 of 23 patients within 20 min-
utes. Sinha and Naritoku [47] reviewed hospital records of 13 elderly pa-
tients with SE and cardiovascular instability who received intravenous
valproate therapy. A loading dose of valproate of 25.1 Æ 5 mg/kg (range
14.7–32.7 mg/kg), at a rate of 36.6 Æ 25.1 mg/min (range 6.3–100 mg/min), was used. There were no significant changes in blood pressure, pulse,
or increases of vasopressor dosages. All patients died as a result of their un-
derlying medical illness or withdrawal of life support. Peters and Pohlmann-
Eden [48] reported a series of 102 adult patients who received standardized
high-dose intravenous VPA in various situations, including 35 patients who
were in SE; 85.6% had interruption of clinical seizure activity within less
than 15 minutes, followed by freedom from seizure during intravenous ther-
apy for at least 12 hours. Subgroup analysis showed efficacy of intravenous
VPA in 27 of 35 patients with SE (77.1%). None had serious side eff ects, in-cluding sedation or hypotension.
Adverse eff ects from valproate include hyperammonemic encephalopa-
thy, pancreatitis, parkinsonism, rare liver failure, and not-so-rare thrombo-
cytopenia, which is usually dose related and benign. Other types of
VPA-associated bleeding diathesis have been observed, including platelet
dysfunction and hypofibrinogenemia.
647SEIZURES AND STATUS EPILEPTICUS

8/8/2019 Avances en el tratamiento del estado epil+®ptico en el paciente cr+¡tico (2007)
http://slidepdf.com/reader/full/avances-en-el-tratamiento-del-estado-epilptico-en-el-paciente-crtico 12/23
If seizures persist, intubation becomes required if not performed yet, and
continuous intravenous drugs become necessary to control the SE. Only
a few agents are available for control of refractory SE, and no consensushas been reached regarding the degree or duration of the required EEG sup-
pression. In a retrospective review, Rossetti and coworkers [49] showed that
achievement of burst suppression on EEG did not correlate with a better
outcome. Further studies are needed to evaluate the relationships between
the depth of burst suppression, duration of therapy, and outcomes. Claassen
and colleagues [50] did a systematic review of the literature on use of pento-
barbital, propofol, and midazolam in refractory SE and found that most pa-
tients already had been treated with phenytoin, benzodiazepines, and
phenobarbital before continuous intravenous therapy. Duration of infusionwas longest with midazolam and shortest with pentobarbital. Continuous
EEG monitoring was performed significantly less often in patients treated
with pentobarbital (27%) than in patients treated with midazolam or pro-
pofol, possibly explaining its seemingly higher efficacy. Continuous EEG
is recommended because most seizures in patients with refractory SE are
nonconvulsive and unnoticeable at the bedside [14]. Commonly used thera-
pies for refractory SE include the following.
BarbituratesBarbiturates are direct GABA agonists. Eff ects of barbiturates include
cerebral and respiratory depression, myocardial depression, vasodilation,
hypotension, and ileus. Administration of continuous intravenous barbitu-
rates requires support with mechanical ventilation, intravenous fluids and
vasopressors, and continuous EEG monitoring (or frequent prolonged
checks if continuous EEG is unavailable) to identify breakthrough seizures
and to assess the level of suppression.
Thiopental is one the most preferred drugs for treating SE in the ICU in
the United Kingdom after failure of the initial treatment [51]. The recom-mended dose is 2 to 4 mg/kg bolus, followed by infusion of 3 to 5 mg/kg/h,
although higher doses commonly are used. Thiopental is metabolized by the
liver and should be withdrawn slowly 24 hours after resolution of electro-
graphic seizures. At serum levels less than 30 mg/L, the elimination half-
life is 3 to 11 hours, but this may increase to 60 hours with higher serum
levels and result in a prolonged recovery time.
Pentobarbital has a slower action than thiopental, but cerebral concen-
trations are maintained longer. The loading dose is 5 mg/kg and should
be repeated until seizures stop, with a maximum bolus rate of 25 to50 mg/min. Infusion rates are 0.5 to 10 mg/kg/h, traditionally titrated to
burst suppression on EEG. In some patients, seizures still can occur from
a suppression-burst background, and in other patients seizures are fully
controlled without reaching suppression burst. The half-life is 20–30 hours.
On drug withdrawal, seizures may recur. Although not clearly investigated,
several paroxysmal or periodic patterns on the ictal-interictal continuum
648 ABOU KHALED & HIRSCH
8/8/2019 Avances en el tratamiento del estado epil+®ptico en el paciente cr+¡tico (2007)
http://slidepdf.com/reader/full/avances-en-el-tratamiento-del-estado-epilptico-en-el-paciente-crtico 13/23
have been observed on EEG on withdrawal; these patterns sometimes
resolve without intervention as the withdrawal of barbiturate continues.
Benzodiazepines
Midazolam, which also acts on the GABA-A receptor, is increasingly
used as an alternative to intravenous barbiturates because it is shorter acting
and causes fewer hemodynamic disturbances. The recommended loading
dose is 0.2 mg/kg, and boluses should be repeated every 5 minutes until sei-
zures stop, up to a maximum total loading dose of 2 to 3 mg/kg. The initial
rate is 0.1 mg/kg/h with a continuous dose range of 0.05 to 2.9 mg/kg/h (this
is higher than in older literature, and even higher doses are occasionally
used). The elimination half-life is 1.5 to 3.5 hours initially; with prolonged
use, there may be tolerance, tachyphylaxis, and significant prolongation of
half-life, up to days. Naritoku and Sinha [52] reported slow clearance of
midazolam in two patients after several days of continuous therapy, proba-
bly related to accumulation of midazolam in peripheral compartments
(adipose tissue) with subsequent redistribution back to the central compart-
ment. The time to stop SE is usually less than 1 hour with a duration of
eff ect lasting minutes to hours. Respiratory depression and hypotension are
common side eff ects.
Propofol
Also a GABA-A receptor agonist, propofol has a rapid onset of action of
less than 3 minutes, quick redistribution into body compartments, and easy
reversibility, which has led to widespread use for the sedation of critically ill
patients. The recommended dose for SE is a bolus of 1 to 2 mg/kg, followed
by a continuous infusion of 1 to 15 mg/kg/h with a recommended maximum
dosage of 5 mg/kg/h if used for any length of time There is no consensus
regarding total duration of induced coma when seizures are controlled,but 12 to 24 hours seems to be the most commonly used duration. Side ef-
fects include respiratory depression, hypotension, bradycardia, and the
more recently recognized ‘‘propofol infusion syndrome,’’ consisting of met-
abolic acidosis, cardiac failure, rhabdomyolysis, hypotension, and death. In
2001, the US Food and Drug Administration communicated that pediatric
ICU patients given propofol for sedation had higher death rates that pa-
tients who received other standard anesthetic agents. In recent years, case
reports regarding propofol infusion syndrome in adults also have emerged.
Risk factors were mostly prolonged infusion (O48 hours), high doses(O5mg/kg/h) [53,54], severe head injury [55], lean mass, and concurrent
use of catecholamines or steroids [54]. It has been suggested that concomi-
tant use of propofol with catecholamines may precipitate this syndrome.
Cray [56] proposed that either propofol or its lipid soluent aff ects cellular
metabolism, causing a biochemical break in the respiratory chain that leads
to lactic acidosis and multiple organ dysfunction. It is prudent to avoid
649SEIZURES AND STATUS EPILEPTICUS
8/8/2019 Avances en el tratamiento del estado epil+®ptico en el paciente cr+¡tico (2007)
http://slidepdf.com/reader/full/avances-en-el-tratamiento-del-estado-epilptico-en-el-paciente-crtico 14/23
prolonged use of propofol (O48 hours) at higher doses (O5 mg/kg/h), and
once used, the authors recommend close monitoring of creatine kinase and
lactic acid. Rossetti and colleagues [57] used concomitant intravenous clona-zepam and propofol at the lowest eff ective dose. In their group of 31 pa-
tients with refractory SE, none had evidence of propofol infusion
syndrome, and only one had isolated hyperlipidemia. Overall mortality
was 22%, which is low for patients with refractory SE, and there were no
neurologic sequelae in 20 of the 25 patients who survived. This was the first
published series of SE patients treated with propofol who did not have very
high mortality.
Other antiepileptic drugsIn recent years, there has been increasing use of enterally administered lev-
etiracetam in ICU patients. Levetiracetam, whose mechanism of action is not
well understood, has the advantages of rapid titration and a good safety pro-
file. It is less than 10% protein bound, with a plasma half-life of 6 to 8 hours. It
is not metabolized by the liver, making it an excellent choice (as are gabapentin
and pregabalin) in patients with hepatic failure. Dosage should be reduced in
the presence of renal impairment, and supplemental doses should be given af-
ter dialysis (approximately 50% of the pool of levitiracetam in the body is re-
moved during a standard 4-hour hemodialysis procedure).There are onlya few reports on its use in SE [58,59]. An intravenous formulation of levetira-
cetam is expected to be available shortly.
Topiramate, administered via the nasogastic route, is reported to be eff ec-
tive in aborting SE [60], possibly owing to the multiple mechanisms of ac-
tion. There is evidence of a neuroprotective eff ect of topiramate, with
attenuation of seizure-induced neuronal injury noted in experimental SE
[61]. Several other oral AEDs have been used for refractory seizures or
SE in the ICU, but there are no comparative data to help select one over
the other. If topiramate or zonisamide is used, one should remain vigilantfor metabolic acidosis (particularly in combination with propofol) because
they are both carbonic anhydrase inhibitors. If carbamazepine or oxcarba-
zepine is used, one should be attentive to hyponatremia.
Ketamine is an anesthetic and NMDA receptor antagonist that has been
used in refractory SE with success in animal models [62–64]. Borris and as-
sociates [62] showed that in contrast to its failure to control early SE, ket-
amine is more eff ective in treatment of prolonged SE, the opposite of
phenobarbital in an animal model of SE (rats who underwent electrical stim-
ulation of the hippocampus). There is evidence that it also may be an ago-nist at the GABA-A receptor [64], that it has neuroprotective eff ects, and
that it does not compromise the hemodynamic status of ICU patients. A
few case reports have been reported in humans [65,66], but no clear evidence
supports its use in SE at this point. Severe neurotoxicity has been reported
secondary to NMDA-receptor antagonism, so further studies and extreme
caution are needed before its widespread use in SE.
650 ABOU KHALED & HIRSCH

8/8/2019 Avances en el tratamiento del estado epil+®ptico en el paciente cr+¡tico (2007)
http://slidepdf.com/reader/full/avances-en-el-tratamiento-del-estado-epilptico-en-el-paciente-crtico 15/23
The efficacy of isoflurane, an inhalational anesthetic agent, in aborting sei-
zures in nine patients with refractory SE was shown in a report by Kofke and
colleagues [67], who also noted that seizures could recur on discontinuation.They recommended its use only when other agents have failed. Mirsattari
and colleagues [68] described seven patients with refractory SE who received
isoflurane with or without desflurane with a goal of burst suppression on
EEG to control SE. Four patients had good outcomes, and three died; all ex-
perienced hypotension. Other complications included atelectasis and ileus.
Steroids, intravenous immunoglobulins, plasmapheresis, and adrenocor-
ticotropic hormone all have been reported to help control seizures, mostly in
the pediatric population or as part of syndromes known to involve immune
mechanisms. More research is needed to clarify the indications and conse-quences of each of these therapies [69].
Extensively used in cardiology, lidocaine’s main advantages are a short
half-life and a relative lack of respiratory and cerebral depressant eff ects.
It is 65% protein bound with a distribution half-life of less than 10 minutes
in adults and rapid hepatic metabolism. Pascual and colleagues [70] reported
42 episodes of SE treated with a lidocaine intravenous bolus dose of 1.5 to
2 mg/kg over 2 minutes; 31 responded to the first injection, but seizures re-
curred in 19. Eleven were nonresponders to the first and second bolus. Ef-
fects are thought to be temporary because of its rapid clearance. It isuseful as a short-term AED, particularly in patients with preexisting respi-
ratory disease as an alternative to benzodiazepines. Toxic eff ects include hy-
potension, sedation, and other neurologic side eff ects such as hallucinations
or exacerbation of seizures.
Acute seizures in special intensive care situations
Seizures and liver disease
The reported incidence of seizures in liver failure ranges from 2% to 33%[71]. Postulated pathophysiologic factors include hyperammonemia; abnor-
mal glutamine metabolism; cerebral ischemia; cerebral edema; accumulation
of toxins; or associated biochemical abnormalities such as hyponatremia,
hypomagnesemia; and renal failure [72–74]. Elevation of endogenous benzo-
diazepines may lower the incidence of seizures in hepatic failure.
Ficker and coworkers [73] reviewed EEGs of 118 patients with hepatic
encephalopathy and identified epileptiform abnormalities in 15%. Twelve
patients had clinical seizures, and most of them died or deteriorated. There
are rare reports of SE [74]. It is important to detect subclinical ictal activityin these patients because seizures increase cerebral oxygen requirements and
may worsen brain edema and prognosis. Ellis and colleagues [72] evaluated
42 patients in grade III or IV hepatic encephalopathy using a bedside cere-
bral function and activity monitor (two-channel, five-lead EEG designed to
study background activity, not seizures). Twenty patients were given phe-
nytoin, and 22 acted as controls. Subclinical seizure activity was reported
651SEIZURES AND STATUS EPILEPTICUS

8/8/2019 Avances en el tratamiento del estado epil+®ptico en el paciente cr+¡tico (2007)
http://slidepdf.com/reader/full/avances-en-el-tratamiento-del-estado-epilptico-en-el-paciente-crtico 16/23
in 3 (15%) and 10 (45%) patients of the treated and control groups, respec-
tively. Autopsy examinations available in 19 patients showed signs of cere-
bral edema in only 22% of the phenytoin-treated patients compared with70% of the controls (P ! .033). This study emphasizes the importance of
continuous brain monitoring in the critically ill as outlined earlier, although
we recommend performing EEG with a full set of electrodes to allow accu-
rate diagnosis and diff erentiation of seizures from other patterns, such as tri-
phasic waves, artifact, and high-voltage slowing. Even with a full set of
electrodes and board-certified epilepsy specialists, this diff erentiation can
be challenging or impossible [31,75–77].
The overall therapeutic approach of seizures and SE in these patients
does not diff er from others except that special considerations should bemade with use of AEDs metabolized by the liver. The degree of hepatic fail-
ure might aff ect the AEDs’ metabolism; in early hepatitis, there may be in-
creased blood flow to the liver with relatively normal hepatic function,
a situation that may increase hepatic clearance of the drugs. In more
advanced hepatic failure with necrosis, hepatocellular tissue decreases, and
serum levels of drugs cleared by the liver may increase [78]. Hypoalbumine-
mia, also encountered in malnutrition and infectious, renal, or neoplastic
diseases, can lead to increased free blood levels of some AEDs that are
highly bound to protein, such as phenytoin and VPA. Monitoring free levelsof these drugs, especially phenytoin, avoids toxicity (which can include
worsening encephalopathy and myoclonus). Other AEDs favored in this sit-
uation would be drugs with low or no protein binding eff ect or with primar-
ily renal metabolism, such as gabapentin, pregabalin, and levetiracetam. To
this date, these drugs are available only in the oral form, but an intravenous
form of levetiracetam is expected to be available soon. In a study in animal
models, Gibbs and associates [79] showed that levetiracetam has neuropro-
tective eff ect against mitochondrial dysfunction and oxidative stress seen
after SE. This eff ect also has been reported with topiramate [61,80], butfurther studies are needed for both of these agents.
Seizures and renal disease
Acute renal failure is associated with uremic encephalopathy and
seizures, which may result from metabolic abnormalities, such as hyponatre-
mia, calcium disorders, uremia, hypertensive encephalopathy, or dysequili-
brium syndrome seen with hemodialysis. The incidence of seizures in
patients undergoing hemodialysis for renal failure has been estimated at
2% to 10% [81–83].Treatment of these patients may be problematic because of alteration of
AED pharmacokinetics in uremia, decreased albumin, and dialysis eff ects.
AEDs predominantly eliminated by the kidneys, such as gabapentin, prega-
balin, and levetiracetam in particular, but also topiramate and phenobarbi-
tal, should be used at much lower doses in renal failure. Some carbonic
anhydrase inhibitors, such as zonisamide and topiramate, should be avoided
652 ABOU KHALED & HIRSCH

8/8/2019 Avances en el tratamiento del estado epil+®ptico en el paciente cr+¡tico (2007)
http://slidepdf.com/reader/full/avances-en-el-tratamiento-del-estado-epilptico-en-el-paciente-crtico 17/23
in patients at risk of nephrolithiasis or when the etiology of the renal failure
is unknown because they increase renal bicarbonate loss and stone forma-
tion. As far as dialysis eff ects, drugs that are highly protein bound (phenyt-oin, valproate, tiagabine; moderately high binding with carbamazepine) are
not dialyzed significantly (although the unbound portion is higher than
usual in these patients, so the eff ect is unpredictable) and do not usually
need to be replaced. Some AEDs are moderately aff ected (lamotrigine,
55% protein bound, 20% dialyzable) and might require predialysis and
postdialysis level monitoring to make necessary adjustments (postdialysis
supplementation). AEDs requiring replacement after dialysis are gabapen-
tin, pregabalin, ethosuximide, levetiracetam, phenobarbital, and topiramate.
In general, the serum concentration of these AEDs decreases by 50% afterdialysis.
Seizures in transplant patients
Seizures in transplant patients are frequent and may arise from metabolic
abnormalities such as hyponatremia, hyperglycemia or hypoglycemia, neu-
rotoxicity from immunosuppressive agents or other medications (eg, high-
dose intravenous antibiotics), infections including brain abscess, cerebral
edema, cerebral infarction, or postanoxic encephalopathy secondary to hy-
povolemia or septic shock [84,85]. The incidence of seizures in transplant pa-tients varies depending on the transplanted organ (Table 2), but the true
proportion is likely underestimated because none of the studies done so
far used continuous EEG in these patients to rule out nonconvulsive sei-
zures. Some of the reports include encephalopathy as a neurologic compli-
cation after transplant without clarifying EEG findings.
One third of liver transplant patients are believed to have seizures
[86,87]. Wijdicks and coworkers [88] reviewed 630 orthotopic liver transplant
recipients and found generalized tonic clonic seizures in 28 (4%), none of
whom had history of seizures before the transplant. Most seizures in criticallyill patients are now known to be nonconvulsive [9,13,14,89]; thus, this is likely
an underestimation of the prevalence of seizures in these patients. Most seizures
occurred in the postoperative period, usually on days 4 to 6 (raising the pos-
sibility that ‘‘withdrawl’’ from high levels of endogenus benzodiazepines plays
a role). Phenytoin eff ectively treated clinical seizures in all 28 patients and was
Table 2
Seizures after transplantation
Organ transplanted Incidence of seizures (%)
Liver 25 [86] –30 [87]
Kidney 1 [94] –5 [95] –31 [96]
Heart 2 [97,98] –6.5 [99] –15 [100]
Lung 22 [101] –27 [102]
Bone marrow 3 [103] –7.5 [104] –12.5 [105]
Pancreas 13 [106]
653SEIZURES AND STATUS EPILEPTICUS

8/8/2019 Avances en el tratamiento del estado epil+®ptico en el paciente cr+¡tico (2007)
http://slidepdf.com/reader/full/avances-en-el-tratamiento-del-estado-epilptico-en-el-paciente-crtico 18/23
successfully discontinued in all survivors shortly thereafter. Immunosuppres-
sant drug neurotoxicity is the most commonly cited etiology, particularly tox-
icity associated with the calcineurin inhibitors cyclosporine and tacrolimus.These agents are linked to a wide spectrum of neurologic abnormalities, partic-
ularly in liver transplant patients, including tremor, visual hallucinations,
speech difficulties, cortical blindness, posterior cerebral edema (also known
as posterior reversible encephalopathy syndrome), and seizures. Factors that
may promote the development of serious complications include advanced liver
failure, hypertension, hypocholesterolemia, elevated cyclosporine or tacroli-
mus blood levels, and hypomagnesemia. Nonconvulsive SE should be consid-
ered in the diff erential diagnosis of delirium and agitation in the post-transplant
period, and continuous EEG monitoring should be obtained. (A 30- to 60-min-ute EEG would detect only one third to one half of cases with nonconvulsive
seizures [14,89].) In cardiac transplant patients, AEDs should be used with cau-
tion owing to the risks of arrhythmias (phenytoin, carbamazepine), hyponatre-
mia (carbamazepine, oxcarbamazepine), and cardiovascular depression
(phenobarbital).
Anticonvulsant use is valuable in the short-term, but data are unclear re-
garding duration of treatment. This should be decided on a case-by-case basis
depending on the etiology and the radiologic and electrographic findings. If
there is an acute symptomatic explanation for seizures that has been corrected,there is no indication for prolonged AED use. In liver transplant patients,
phenytoin may be needed for rapid seizure control, and levetiracetam also
may be used as discussed earlier. Gabapentin, pregabalin, and topiramate
are other agents that can be advanced relatively fast.
Medication interactions constitute another concern in the transplant pop-
ulation. Phenytoin decreases absorption of cyclosporine [90], and all hepatic
enzyme inducers (including phenytoin, carbamazpine, and phenobarbital)
can increase the clearance of cyclosporine, methylprednisolone, and many
other medications dramatically.
Summary
Seizures occur in critically ill patients in variable conditions. In all situa-
tions, it is crucial to identify potential causes or contributors, particularly
reversible factors, such as metabolic disturbances, fever, hypoxia, and med-
ications. For SE, it is imperative to begin treatment as soon as possible and
to treat until success is verified with EEG or the patient returns to normal
mental status.Nonconvulsive seizures are underdiagnosed. Most seizures in critically ill
patients are nonconvulsive and can be detected only with EEG monitoring.
The authors recommend continuous EEG monitoring in critically ill pa-
tients with alteration of mental status, especially if there is concurrent acute
brain injury, prior epilepsy, a prior clinical seizure or SE, fluctuating mental
status, coma, abnormal eye movements, or subtle twitching. Nonconvulsive
654 ABOU KHALED & HIRSCH
8/8/2019 Avances en el tratamiento del estado epil+®ptico en el paciente cr+¡tico (2007)
http://slidepdf.com/reader/full/avances-en-el-tratamiento-del-estado-epilptico-en-el-paciente-crtico 19/23
seizures are associated with additional neuronal metabolic stress, increased
edema or mass eff ect, and worse clinical outcome. Future studies are needed
to determine whether greater use of EEG monitoring and early or more ag-gressive treatment of nonconvulsive seizures would improve the outcome of
these patients.
References
[1] DeLorenzo RJ, Pellock JM, Towne AR, et al. Epidemiology of status epilepticus. J Clin
Neurophysiol 1995;12:316–25.
[2] Gastaut H. Classification of status epilepticus. Adv Neurol 1983;34:15–35.
[3] Bleck TP. Convulsive disorders: status epilepticus. Clin Neuropharmacol 1991;14:191–8.
[4] Lowenstein DH, Bleck T, Macdonald RL. It’s time to revise the definition of status epilep-
ticus. Epilepsia 1999;40:120–2.
[5] Treiman DM, Meyers PD, Walton NY, et al. A comparison of four treatments for gener-
alized convulsive status epilepticus. Veterans Aff airs Status Epilepticus Cooperative Study
Group. N Engl J Med 1998;339:792–8.
[6] Lowenstein DH, Alldredge BK. Status epilepticus at an urban public hospital in the 1980s.
Neurology 1993;43(3 Pt 1):483–8.
[7] Towne AR, Waterhouse EJ, Boggs JG, et al. Prevalence of nonconvulsive status epilepticus
in comatose patients. Neurology 2000;54:340–5.
[8] Koppel BS, Hauser WA, Politis C, et al. Seizures in the critically ill: the role of imipenem.
Epilepsia 2001;42:1590–3.
[9] Hirsch LJ, Claassen J. The current state of treatment of status epilepticus. Curr Neurol
Neurosci Rep 2002;2:345–56.
[10] Kaplan PW. The clinical features, diagnosis, and prognosis of nonconvulsive status epilep-
ticus. Neurologist 2005;11:348–61.
[11] DeLorenzo RJ, Waterhouse EJ, Towne AR, et al. Persistent nonconvulsive status epilepti-
cus after the control of convulsive status epilepticus. Epilepsia 1998;39:833–40.
[12] Jordan K. Nonconvulsive status epilepticus in acute brain injury. J Clin Neurophysiol 1999;
16:332–40.
[13] Vespa PM, Nuwer MR, Nenov V, et al. Increased incidence and impact of nonconvulsive
and convulsive seizures after traumatic brain injury as detected by continuous electroen-cephalographic monitoring. J Neurosurg 1999;91:750–60.
[14] Claassen J, Mayer SA, Kowalski RG, et al. Detection of electrographic seizures with con-
tinuous EEG monitoring in critically ill patients. Neurology 2004;62:1743–8.
[15] Hesdorff er DC, Logroscino G, Cascino G, et al. Incidence of status epilepticus in Roches-
ter, Minnesota, 1965–1984. Neurology 1998;50:735–41.
[16] DeLorenzo RJ, Hauser WA, Towne AR, et al. A prospective, population-based epidemio-
logic study of status epilepticus in Richmond, Virginia. Neurology 1996;46:1029–35.
[17] DeLorenzo RJ, Towne AR, Pellock JM, et al. Status epilepticus in children, adults, and the
elderly. Epilepsia 1992;33(Suppl 4):S15–25.
[18] Towne AR, Pellock JM, Ko D, et al. Determinants of mortality in status epilepticus.
Epilepsia 1994;35:27–34.[19] Litt B, Wityk RJ, Hertz SH, et al. Nonconvulsive status epilepticus in the critically ill
elderly. Epilepsia 1998;39:1194–202.
[20] Shneker BF, Fountain NB. Assessment of acute morbidity and mortality in nonconvulsive
status epilepticus. Neurology 2003;61:1066–73.
[21] Lothman EW, Bertram EH, Bekenstein JW, et al. Self-sustaining limbic status epilepticus
induced by ‘continuous’ hippocampal stimulation: electrographic and behavioral charac-
teristics. Epilepsy Res 1989;3:107–19.
655SEIZURES AND STATUS EPILEPTICUS
8/8/2019 Avances en el tratamiento del estado epil+®ptico en el paciente cr+¡tico (2007)
http://slidepdf.com/reader/full/avances-en-el-tratamiento-del-estado-epilptico-en-el-paciente-crtico 20/23
[22] Sankar R, Shin DH, Wasterlain CG. Serum neuron-specific enolase is a marker for neuro-
nal damage following status epilepticus in the rat. Epilepsy Res 1997;28:129–36.
[23] DeGiorgio CM, Correale JD, Gott PS, et al. Serum neuron-specific enolase in human status
epilepticus. Neurology 1995;45:1134–7.
[24] DeGiorgio CM, Heck CN, Rabinowicz AL, et al. Serum neuron-specific enolase in the
major subtypes of status epilepticus. Neurology 1999;52:746–9.
[25] DeGiorgio CM, Gott PS, Rabinowicz AL, et al. Neuron-specific enolase, a marker of acute
neuronal injury, is increased in complex partial status epilepticus. Epilepsia 1996;37:606–9.
[26] Rabinowicz AL, Correale JD, Bracht KA, et al. Neuron-specific enolase is increased after
nonconvulsive status epilepticus. Epilepsia 1995;36:475–9.
[27] Kim JA, Chung JI, Yoon PH, et al. Transient MR signal changes in patients with general-
ized tonicoclonic seizure or status epilepticus: periictal diff usion-weighted imaging. AJNR
Am J Neuroradiol 2001;22:1149–60.
[28] Wieshmann UC, Woermann FG, Lemieux L, et al. Development of hippocampal atrophy:
a serial magnetic resonance imaging study in a patient who developed epilepsy after gener-
alized status epilepticus. Epilepsia 1997;38:1238–41.
[29] Chan S, Chin SS, Kartha K, et al. Reversible signal abnormalities in the hippocampus and
neocortex after prolonged seizures. AJNR Am J Neuroradiol 1996;17:1725–31.
[30] DeGiorgio CM, Tomiyasu U, Gott PS, et al. Hippocampal pyramidal cell loss in human
status epilepticus. Epilepsia 1992;33:23–7.
[31] Fountain NB, Lothman EW. Pathophysiology of status epilepticus. J Clin Neurophysiol
1995;12:326–42.
[32] Simon RP. Physiologic consequences of status epilepticus. Epilepsia 1985;26(Suppl 1):
S58–66.
[33] Meldrum BS, Vigouroux RA, Brierley JB. Systemic factors and epileptic brain damage:prolonged seizures in paralyzed, artificially ventilated baboons. Arch Neurol 1973;29:82–7.
[34] Boggs JG, Painter JA, DeLorenzo RJ. Analysis of electrocardiographic changes in status
epilepticus. Epilepsy Res 1993;14:87–94.
[35] Manno EM, Pfeifer EA, Cascino GD, et al. Cardiac pathology in status epilepticus. Ann
Neurol 2005;58:954–7.
[36] Chen DK, So YT, Fisher RS. Use of serum prolactin in diagnosing epileptic seizures: report
of the Therapeutics and Technology Assessment Subcommittee of the American Academy
of Neurology. Neurology 2005;65:668–75.
[37] Barry E, Hauser WA. Pleocytosis after status epilepticus. Arch Neurol 1994;51:190–3.
[38] Aminoff MJ, Simon RP. Status epilepticus: causes, clinical features and consequences in 98
patients. Am J Med 1980;69:657–66.[39] Mazarati AM, Baldwin RA, Sankar R, et al. Time-dependent decrease in the eff ectiveness
of antiepileptic drugs during the course of self-sustaining status epilepticus. Brain Res 1998;
814(1–2):179–85.
[40] Bleck TP. Management approaches to prolonged seizures and status epilepticus. Epilepsia
1999;40(Suppl 1):S59–63.
[41] Leppik IE, Derivan AT, Homan RW, et al. Double-blind study of lorazepam and diazepam
in status epilepticus. JAMA 1983;249:1452–4.
[42] Pang T, Hirsch LJ. Treatment of convulsive and nonconvulsive status epilepticus. Curr
Treat Options Neurol 2005;7:247–59.
[43] Bauer LA. Interference of oral phenytoin absorption by continuous nasogastric feedings.
Neurology 1982;32:570–2.[44] Sander JW, Perucca E. Epilepsy and comorbidity: infections and antimicrobials usage in
relation to epilepsy management. Acta Neurol Scand Suppl 2003;180:16–22.
[45] Czapinski P, Terczynski A. [Intravenous valproic acid administration in status epilepticus].
Neurol Neurochir Pol 1998;32:11–22.
[46] Giroud M, Gras D, Escousse ADR, et al. Use of injectable valproic acid in status epilepti-
cus: a pilot study. Drug Invest 1993;5:154–9.
656 ABOU KHALED & HIRSCH

8/8/2019 Avances en el tratamiento del estado epil+®ptico en el paciente cr+¡tico (2007)
http://slidepdf.com/reader/full/avances-en-el-tratamiento-del-estado-epilptico-en-el-paciente-crtico 21/23
[47] Sinha S, Naritoku DK. Intravenous valproate is well tolerated in unstable patients with
status epilepticus. Neurology 2000;55:722–4.
[48] Peters CN, Pohlmann-Eden B. Intravenous valproate as an innovative therapy in seizure
emergency situations including status epilepticusd
experience in 102 adult patients. Seizure
2005;14:164–9.
[49] Rossetti AO, Logroscino G, Bromfield EB. Refractory status epilepticus: eff ect of treat-
ment aggressiveness on prognosis. Arch Neurol 2005;62:1698–702.
[50] Claassen J, Hirsch LJ, Emerson RG, et al. Treatment of refractory status epilepticus with
pentobarbital, propofol, or midazolam: a systematic review. Epilepsia 2002;43:146–53.
[51] Walker MC, Smith SJ, Shorvon SD. The intensive care treatment of convulsive status epi-
lepticus in the UK: results of a national survey and recommendations. Anaesthesia 1995;50:
130–5.
[52] Naritoku DK, Sinha S. Prolongation of midazolam half-life after sustained infusion for sta-
tus epilepticus. Neurology 2000;54:1366–8.
[53] Vasile B, Rasulo F, Candiani A, et al. The pathophysiology of propofol infusion syndrome:
a simple name for a complex syndrome. Intensive Care Med 2003;29:1417–25.
[54] Kumar MA, Urrutia VC, Thomas CE, et al. The syndrome of irreversible acidosis after pro-
longed propofol infusion. Neurocrit Care 2005;3:257–9.
[55] Cremer OL, Moons KG, Bouman EA, et al. Long-term propofol infusion and cardiac fail-
ure in adult head-injured patients. Lancet 2001;357:117–8.
[56] Cray S. Fat metabolism during propofol infusion. Br J Anaesth 1999;82:473.
[57] Rossetti AO, Reichhart MD, Schaller MD, et al. Propofol treatment of refractory status
epilepticus: a study of 31 episodes. Epilepsia 2004;45:757–63.
[58] Rossetti AO, Bromfield EB. Levetiracetam in the treatment of status epilepticus in adults:
a study of 13 episodes. Eur Neurol 2005;54:34–8.[59] Rossetti AO, Bromfield EB. Determinants of success in the use of oral levetiracetam in sta-
tus epilepticus. Epilepsy Behav 2006;8:651–4.
[60] Towne AR, Garnett LK, Waterhouse EJ, et al. The use of topiramate in refractory status
epilepticus. Neurology 2003;60:332–4.
[61] Niebauer M, Gruenthal M. Topiramate reduces neuronal injury after experimental status
epilepticus. Brain Res 1999;837:263–9.
[62] Borris DJ, Bertram EH, Kapur J. Ketamine controls prolonged status epilepticus. Epilepsy
Res 2000;42:117–22.
[63] Guler G, Erdogan F, Golgeli A, et al. Ketamine reduces lidocaine-induced seizures in mice.
Int J Neurosci 2005;115:1239–44.
[64] Irifune M, Sato T, Kamata Y, et al. Evidence for GABA(A) receptor agonistic properties of ketamine: convulsive and anesthetic behavioral models in mice. Anesth Analg 2000;91:
230–6.
[65] Mewasingh LD, Sekhara T, Aeby A, et al. Oral ketamine in paediatric non-convulsive sta-
tus epilepticus. Seizure 2003;12:483–9.
[66] Ubogu EE, Sagar SM, Lerner AJ, et al. Ketamine for refractory status epilepticus: a case of
possible ketamine-induced neurotoxicity. Epilepsy Behav 2003;4:70–5.
[67] Kofke WA, Young RS, Davis P, et al. Isoflurane for refractory status epilepticus: a clinical
series. Anesthesiology 1989;71:653–9.
[68] Mirsattari SM, Sharpe MD, Young GB. Treatment of refractory status epilepticus with in-
halational anesthetic agents isoflurane and desflurane. Arch Neurol 2004;61:1254–9.
[69] Prasad AN, Stafstrom CF, Holmes GL. Alternative epilepsy therapies: the ketogenic diet,immunoglobulins, and steroids. Epilepsia 1996;37(Suppl 1):S81–95.
[70] Pascual J, Ciudad J, Berciano J. Role of lidocaine (lignocaine) in managing status epilepti-
cus. J Neurol Neurosurg Psychiatry 1992;55:49–51.
[71] Plum FPJ. Diagnosis of stupor and coma. Philadelphia: Davis; 1984.
[72] Ellis AJ, Wendon JA, Williams R. Subclinical seizure activity and prophylactic phenytoin
infusion in acute liver failure: a controlled clinical trial. Hepatology 2000;32:536–41.
657SEIZURES AND STATUS EPILEPTICUS
8/8/2019 Avances en el tratamiento del estado epil+®ptico en el paciente cr+¡tico (2007)
http://slidepdf.com/reader/full/avances-en-el-tratamiento-del-estado-epilptico-en-el-paciente-crtico 22/23
[73] Ficker DM, Westmoreland BF, Sharbrough FW. Epileptiform abnormalities in hepatic
encephalopathy. J Clin Neurophysiol 1997;14:230–4.
[74] Eleftheriadis N, Fourla E, Eleftheriadis D, et al. Status epilepticus as a manifestation of
hepatic encephalopathy. Acta Neurol Scand 2003;107:142–4.
[75] Chong DJ, Hirsch LJ. Which EEG patterns warrant treatment in the critically ill? Review-
ing the evidence for treatment of periodic epileptiform discharges and related patterns.
J Clin Neurophysiol 2005;22:79–91.
[76] Fountain NB, Waldman WA. Eff ects of benzodiazepines on triphasic waves: implications
for nonconvulsive status epilepticus. J Clin Neurophysiol 2001;18:345–52.
[77] Brenner RP. Is it status? Epilepsia 2002;43(Suppl 3):103–13.
[78] Rodighiero V. Eff ects of liver disease on pharmacokinetics: an update. Clin Pharmacokinet
1999;37:399–431.
[79] Gibbs JE, Walker MC, Cock HR. Levetiracetam: antiepileptic properties and protective ef-
fects on mitochondrial dysfunction in experimental status epilepticus. Epilepsia 2006;47:
469–78.
[80] Kudin AP, Debska-Vielhaber G, Vielhaber S, et al. The mechanism of neuroprotection by
topiramate in an animal model of epilepsy. Epilepsia 2004;45:1478–87.
[81] Glenn CM, Astley SJ, Watkins SL. Dialysis-associated seizures in children and adolescents.
Pediatr Nephrol 1992;6:182–6.
[82] Bergen DC, Ristanovic R, Gorelick PB, et al. Seizures and renal failures. Int J Artif Organs
1994;17:247–51.
[83] Scorza FA, Albuquerque M, Arida RM, et al. Seizure occurrence in patients with chronic
renal insufficiency in regular hemodialysis program. Arq Neuropsiquiatr 2005;63:757–60.
[84] Bechstein WO. Neurotoxicity of calcineurin inhibitors: impact and clinical management.
Transpl Int 2000;13:313–26.[85] Wijdicks EF, Wiesner RH, Krom RA. Neurotoxicity in liver transplant recipients with cy-
closporine immunosuppression. Neurology 1995;45:1962–4.
[86] Adams DH, Ponsford S, Gunson B, et al. Neurological complications following liver trans-
plantation. Lancet 1987;1:949–51.
[87] Martinez AJ, Estol C, Faris AA. Neurologic complications of liver transplantation. Neurol
Clin 1988;6:327–48.
[88] Wijdicks EF, Plevak DJ, Wiesner RH, et al. Causes and outcome of seizures in liver trans-
plant recipients. Neurology 1996;47:1523–5.
[89] Pandian JD, Cascino GD, So EL, et al. Digital video-electroencephalographic monitoring
in the neurological-neurosurgical intensive care unit: clinical features and outcome. Arch
Neurol 2004;61:1090–4.[90] Rowland M, Gupta SK. Cyclosporin-phenytoin interaction: re-evaluation using metabolite
data. Br J Clin Pharmacol 1987;24:329–34.
[91] Shuman RE, Varelas PN. Seizure-inducing drugs used for the critically ill. In: Varelas PN,
editor. Seizures in critical care: a guide to diagnosis and therapeutics. Totowa (NJ):
Humana Press; 2005. p. 261–90.
[92] Garcia PA, Alldredge BK. Medication-associated seizures. In: Delanty N, editor. Seizures:
Medical Causes and Management. Totowa (NJ): Humana Press; 2001. p. 147–65.
[93] Garcia PA, Alldredge BK. Drug-induced seizures. Neurol Clin 1994;12:85–99.
[94] Jost L, Jost L, Nogues M, et al. [Neurological complications of renal transplant]. Medicina
(B Aires) 2000;60:161–4.
[95] Veroux P, Veroux M, Puliatti C, et al. Tacrolimus-induced neurotoxicity in kidney trans-plant recipients. Transplant Proc 2002;34:3188–90.
[96] McEnery PT, Nathan J, Bates SR, et al. Convulsions in children undergoing renal trans-
plantation. J Pediatr 1989;115:532–6.
[97] Perez-Miralles F, Sanchez-Manso JC, Almenar-Bonet L, et al. Incidence of and risk factors
for neurologic complications after heart transplantation. Transplant Proc 2005;37:
4067–70.
658 ABOU KHALED & HIRSCH

8/8/2019 Avances en el tratamiento del estado epil+®ptico en el paciente cr+¡tico (2007)
http://slidepdf.com/reader/full/avances-en-el-tratamiento-del-estado-epilptico-en-el-paciente-crtico 23/23
[98] Malheiros SM, Almeida DR, Massaro AR, et al. Neurologic complications after heart
transplantation. Arq Neuropsiquiatr 2002;60:192–7.
[99] Cemillan CA, Alonso-Pulpon L, Burgos-Lazaro R, et al. [Neurological complications in
a series of 205 orthotopic heart transplant patients]. Rev Neurol 2004;38:906–12.
[100] Grigg MM, Costanzo-Nordin MR, Celesia GG, et al. The etiology of seizures after cardiac
transplantation. Transplant Proc 1988;20(Suppl 3):937–44.
[101] Vaughn BV, Ali II, Olivier KN, et al. Seizures in lung transplant recipients. Epilepsia 1996;
37:1175–9.
[102] Wong M, Mallory GB Jr, Goldstein J, et al. Neurologic complications of pediatric lung
transplantation. Neurology 1999;53:1542–9.
[103] Snider S, Bashir R, Bierman P. Neurologic complications after high-dose chemotherapy
and autologous bone marrow transplantation for Hodgkin’s disease. Neurology 1994;44:
681–4.
[104] Furlong TG, Gallucci BB. Pattern of occurrence and clinical presentation of neurological
complications in bone marrow transplant patients. Cancer Nurs 1994;17:27–36.
[105] Antonini G, Ceschin V, Morino S, et al. Early neurologic complications following alloge-
neic bone marrow transplant for leukemia: a prospective study. Neurology 1998;50:1441–5.
[106] Kiok MC. Neurologic complications of pancreas transplants. Neurol Clin 1988;6:367–76.
659SEIZURES AND STATUS EPILEPTICUS