09 Tratamiento combinado de quimio y radioterapia en Cáncer de Pulmón
94
Tratamientos locorregionales en el NSCLC Tratamiento combinado QT/RT B.Massutí Hospital General Universitario Alicante HOSPITALS DÍLLES BALEARS
-
Upload
effyciens-marketing-online-sl -
Category
Health & Medicine
-
view
196 -
download
2
description
Autor/a Dr. Bartomeu Massutí V Jornada de Revisión del Congreso Mundial de Cáncer de Pulmón. ARCO MEDITERRANEO. Valencia 8-Nov-2013
Transcript of 09 Tratamiento combinado de quimio y radioterapia en Cáncer de Pulmón

Tratamientos locorregionales en el NSCLC
Tratamiento combinado QT/RT
B.Massutí
Hospital General Universitario Alicante
BIENVENIDA: Dra. Remei Blanco Guerrero y Dr. Jose Muñoz Langa
10:30. INTRODUCCIÓN: DE AMSTERDAM A SIDNEY
Dra. Remei Blanco
10:45. MESA I: DIAGNÓSTICO, EPIDEMIOLOGÍA Y BIOLOGÍA MOLECULAR.
Moderadores: Dr. Óscar Juan y Dra. Regina Gironés
10:45-11:05. Epidemiología, screening y prevención
Dr. Francisco Aparisi
11:05-11:25. Diagnóstico y estadificación
Dr. César Valdés
11:25-11:45. Biología molecular
Dra. Eloisa Jantús
11:45-12:00. Discusión
12:00-12:15. COFFE BREAK
12:15. MESA II: OTROS TUMORES TORÁCICOS.
Moderadores: Dr. Gaspar Esquerdo y Dr. Josep Belda
12:15-12:30. Mesotelioma y Timoma
Dra. Pilar Lianes
12:30-12:45. SCLC
Dr. Javier Garde
12:45-13:00. Discusión
13:00. MESA III: TRATAMIENTOS LOCORREGIONALES EN EL NSCLC.
Moderadores: Dr. Bartomeu Massutí y Dr. Josep María Solé
13:00-13:15. Cirugía
Dr. José Galbis
13:15-13:30. Radioterapia
Dr. Luis Fernández
13:30-13:45. Tratamiento combinado: QT/RT
Dr. Bartomeu Massuti
13:45-14:00. Discusión
14:00-15:00. COMIDA
15:00. MESA IV: TRATAMIENTOS SISTÉMICOS EN EL NSCLC.
Moderadores: Dra. Edurne Arriola y Dr. Alfredo Sánchez
15:00-15:15. Antiangiogénicos
Dr. Javier Pérez
15:15-15:30. Terapias dirigidas
Dr. Jordi Remón
15:30-15:45. Quimioterapia (1ª y 2ª líneas y mantenimiento)
Dra. Margarita Majem
15:45-16:00. Inumoterapia
Dr. José Muñoz Langa
16:00-16:15. Discusión
16:15. CONCLUSIONES: DE SIDNEY A DENVER
Dra. Josefa Terrasa
CLAUSURA: Dra. Remei Blanco Guerrero y Dr. José Muñoz Langa
HOTEL SILKEN PUERTA VALENCIA ****Cardenal Benlloch, 28
46021-Valencia, España
Tel: +34 963 936 395
PONENTES
Dr. Francisco Aparisi.
Oncología Médica. H. Virgen de Los Lirios. Alcoi.
(Alicante)
Dra. Edurne Arriola.
Oncología Médica. H. del Mar. Barcelona
Dr. Josep Belda.
Cirugía Torácica. H. Mutua de Terrassa. (Barcelona)
Dra. Remei Blanco.
Oncología Médica. H. de Terrassa. (Barcelona)
Dr. Gaspar Esquerdo.
Oncología Médica. H. de Elda. (Alicante)
Dr. Luís Fernández.
Oncología Radioterápica. H. General de Elche. (Alicante)
Dr. José Galbis.
Cirugía Torácica. H. de La Ribera. Alzira (Valencia)
Dr. Javier Garde.
Oncología Médica. H. Arnau de Vilanova. Valencia
Dra. Regina Gironés.
Oncología Médica. H. Lluis Alcanyis. Xátiva (Valencia)
Dra. Eloisa Jantús.
Biología Molecular. H. General Universitario de Valencia
Dr. Óscar Juan Vidal.
Oncología Médica. H. UiP. La Fe. Valencia
Dra. Pilar Lianes.
Oncología Médica. H. de Mataró. (Barcelona)
Dra. Margarita Majem.
Oncología Médica. H. Sant Pau. Barcelona
Dr. Bartomeu Massutí.
Oncología Médica. H. General de Alicante
Dr. José Muñoz Langa.
Oncología Médica. H. Dr. Peset. Valencia
Dr. Javier Pérez.
Oncología Médica. H. General de Elche. (Alicante)
Dr. Jordi Remón.
Oncología Médica. H. de Mataró. (Barcelona)
Dr. Alfredo Sánchez.
Oncología Médica. H. Provincial de Castellón.
Dr. Josep María Solé.
H. General de Cataluña. Bellaterra (Barcelona)
Dra. Josefa Terrassa.
Oncología Médica. H. Son Espases. Palma de Mallorca
Dr. César Valdés.
Neumología. H. de Terrasa. (Barcelona)
HOSPITALS
DÍLLES
BALEARS

Agenda
• Situación actual y resultados terapéuticos
• Cuestiones abiertas
• Presentaciones en WCLC 2013
• Perspectivas de futuros

7th IASLC Staging System
T and M N0 N1 N2 N3
UICC6 and descriptor New
T/M Stg Stg Stg Stg
T1 (2 cm) T1a IA IIA IIIA IIIB
T1 (>2-3 cm) T1b IA IIA IIIA IIIB
T2 (5 cm) T2a IB IIA IIIA IIIB
T2 (>5-7 cm) T2b IIA IIB IIIA IIIB
T2 (>7 cm)
T3
IIB IIIA IIIA IIIB
T3 invasion IIB IIIA IIIA IIIB
T4 (same lobe
nodules) IIB IIIA IIIA IIIB
T4 (extension)
T4
IIIA IIIA IIIB IIIB
M1 (ipsilateral lung) IIIA IIIA IIIB IIIB
T4 (pleural effusion)
M1a
IV IV IV IV
M1 (contralateral
lung) IV IV IV IV
M1 (distant) M1b IV IV IV IV

7th IASLC Staging System
T and M N0 N1 N2 N3
UICC6 and descriptor New
T/M Stg Stg Stg Stg
T1 (2 cm) T1a IA IIA IIIA IIIB
T1 (>2-3 cm) T1b IA IIA IIIA IIIB
T2 (5 cm) T2a IB IIA IIIA IIIB
T2 (>5-7 cm) T2b IIA IIB IIIA IIIB
T2 (>7 cm)
T3
IIB IIIA IIIA IIIB
T3 invasion IIB IIIA IIIA IIIB
T4 (same lobe
nodules) IIB IIIA IIIA IIIB
T4 (extension)
T4
IIIA IIIA IIIB IIIB
M1 (ipsilateral lung) IIIA IIIA IIIB IIIB
T4 (pleural effusion)
M1a
IV IV IV IV
M1 (contralateral
lung) IV IV IV IV
M1 (distant) M1b IV IV IV IV

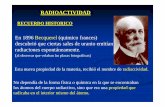
7th IASLC TNM Staging System: Survival according to N status and single/multiple nodal zones

STAGE 5-year SURVIVAL
I 60 – 70%
II 40 – 55%
IIIA 10 – 25%
IIIB 5%
IV < 1%
NSCLC stages at presentation and
treatment outcomes
Approximately 10-15% of newly diagnosed NSCLC p. will be classified as stage IIIA-N2
Stage I
Stage II
Stage III
Stage IV30%

Evolución de los resultados terapéuticos tto QT/RT
• Medianas sup EC aleatorizados:
– 80´s: 9 m
– 90´s: 14 m
– 2000´s: 18 m
– 2010´s: 20 m

Metanálisis QT-RT secuencial vs concomitante / JCO 2010;38:2181-2190

Rowell N; O’Rourke N Cochrane Database Syst Rev 2004
RT vs QTRT (R.R)
Risk of death (2a) 0.93
↑PFS (LR)2a 0.84
↑ PFS 0.90
Absolute risk death 1.13
Anemia 3.19
Neutropenia 3.12
Acute esophagitis 1.58
Late esophagitis 1.72
Pneumonitis 1.19
Lung fibrosis 1.15
QTRTvs QTRT (R.R)
Risk of death (2a) 0.86
↑PFS (LR)2a 0.84
Absolute risk death 1.60
Neutropenia 1.07
Acute esophagitis 6.77
PNeumonitis 0.66

Tratamientos combinación: selección pacientes
Bajo riesgo Riesgo intermedio Alto riesgo
PS 0-1
No comorbilidades
Edad < 70 a
PFR buenas
V20<35%
PS 0-1
Pocas comorbil.
Edad < 80 a
PFR aceptables
35 < V <45%
PS >1
Comorbilidades
Cualquier edad
PFR afectadas
V > 45%
RT-QT concomitante QT-RT secuencial Tratamiento paliat.

Pacientes elegibles para tto QT/RT concomitante
Registro población de Maastricht (853.553 habitantes)
711 pacientes Estadio III (81% CPNM, 18% CPCP) (2002-2005).
Características clínicas: ◦ 545 (76.7%) < 75 años ◦ Comorbilidades: 63.1% (> 75 a) versus 47.1% (< 75 a )
Resultados: ◦ En el grupo de edad 60 – 69 a, solamente 50% se
considerarían elegibles para tto concomitante ◦ Entre 70 – 74 a, < 50% ◦ 60% de la población ineligible para tto concomitante
De Ruysscher D. Ann Oncol 2009

Cuestiones abiertas
• Secuencia QT/RT: – QT Inducción – QT Consolidación
• Esquemas QT concomitante: – Dosis plenas – Dosis frecuentes
• Dosis RT • Integración agentes biológicos • Reducción toxicidad • Estrategias inmunoterapia • Heterogeneidad estadios IIIA-IIIB

RTOG 0617: Phase III Trial of 74 Gy vs 60
Gy RT in Unresectable Stage III NSCLC
Bradley JD, et al. ASCO 2013. Abstract 7501.
*CT consisted of carboplatin/paclitaxel. †400 mg/m2 loading dose on Day 1, followed by weekly dose of 250 mg/m2
Patients with newly
diagnosed, unresectable
stage IIIA/IIIB NSCLC
(N = 464)
Stratified by RT technique,
Zubrod status, PET staging,
histology Concurrent Treatment Consolidation Treatment
Standard-Dose RT + concurrent CT*
(n = 125)
Consolidation CT*
High-Dose RT + concurrent CT*
(n = 121)
Consolidation CT*
Standard-Dose RT + concurrent CT* +
Cetuximab† (n = 108)
Consolidation CT* +
Cetuximab†
High-Dose RT+ concurrent CT* +
Cetuximab† (n = 110)
Consolidation CT* +
Cetuximab†
Primary endpoint: OS

RTOG 0617: Survival
Efficacy Outcome Standard-Dose RT
(n = 213)
High-Dose RT
(n = 206)
HR (95% CI)
P Value
Median OS, mos 28.7 19.5 1.56
(1.19-2.06) .0007
18-mo PFS, % 36.6 26.3 1.30
(1.04-1.63) .0116
18-mo local failure, %
25.1 34.3 1.37
(0.99-1.89) .0319
18-mo distant failure, %
42.4 47.8 1.15
(0.87-1.51) .1576
Bradley JD, et al. ASCO 2013. Abstract 7501.

RTOG 0617: Safety
• Grade 3 esophagitis occurred significantly more often with high-dose vs standard-dose RT (20.9% vs 7.0%; P = .0003)
Adverse Events Definitely, Probably, or Possibly Related to Treatment, %
Standard-Dose RT
(n = 213)
High-Dose RT
(n = 206)
Worst nonhematologic events
Grade 3 46.0 46.1
Grade 4 9.9 11.2
Grade 5 0.9 4.9
Worst overall
Grade 3 46.5 41.7
Grade 4 26.8 31.6
Grade 5 0.9 4.9
Bradley JD, et al. ASCO 2013. Abstract 7501.

Resultados
• HR PFS 0.96 (0.77-1.19)
• HR OS 0.99 (0.78-1.27)

Summary
• High-dose RT (74 Gy) associated with higher risk of death, locoregional recurrence, and incidence of fatal AEs vs low-dose RT (60 Gy) when administered with concurrent CT in patients with newly diagnosed, unresectable stage III NSCLC
• Analysis of the addition of cetuximab to high- and low-dose RT with concurrent CT is ongoing
Bradley JD, et al. ASCO 2013. Abstract 7501.

WCLC 2013: RTOG 0716: Cetuximab analysis
- Compare the overall survival of patients treated with concurrent chemo-radiotherapy plus cetuximab versus chemo-radiotherapy alone










Toxicidades comparativas
Toxicidades Cetuximab (237 p) No Cetuximab (227 p)
Grado 3 Grado 4 Grado 5 Grado 3 Grado 4 Grado 5
No-Hematol. 130 (54.9%)
26 (11%)
11 (4.6%)
91 (40.1%) 18 (7.9%)
6 (2.6%)
Conjunto 167 (70.5%) 115 (50.7%)
Maxima toxicidad
117 (49.4%)
74 (31.2%)
11 (4.6%)
93 (41%)
57 (25.1%) 7 (3.1%)
Conjunto 202 (85.2%) 157 (69.2%)
P> 0.0001

Overall survival













Tecemotide (L-BLP25):
Novel Lipopeptide Cancer Vaccine
Adjuvant = Monophosphoryl lipid A The adjuvant supports T-cell response by inducing pro-inflammatory cytokines (via TLR4 stimulation)
Antigen = BLP25 lipopeptide The amino acids of the lipopeptide provide antigenic epitopes for T cells
MUC1 mucin
Structural lipids = cholesterol, DPPC, and DMPG Further enhancement of antigen delivery/uptake into APCs and immune reaction
G S T A P P A H G V T S A P D T R P A P
S T A P P A H G V T S A P D T R P A P G S T A P P - Lys (PAL) G
Butts CA, et al. ASCO 2013. Abstract 7500. Used with permission.

START: Study Design
Patients with unresectable
stage IIIA/B NSCLC without
disease progression following
chemoradiotherapy
(N = 1239)
Tecemotide 806 µg SC weekly for 8 wks, then every 6 wks thereafter +
Best Supportive Care (n = 829)
Placebo + Best Supportive Care
(n = 410)
Randomized 2:1; stratified by disease stage, response
to chemoradiotherapy, concurrent vs sequential chemoradiotherapy,
geographic region
Treated
until PD
1 dose of cyclophosphamide 300 mg/m2 or saline given 3 days prior to first tecemotide or placebo dose,
respectively.
Butts CA, et al. ASCO 2013. Abstract 7500. Used with permission.

L-BLP25 (n = 829)
Placebo (n = 410)
Median OS, mos 25.6 22.3
Adjusted HR 0.88 (95% CI: 0.75-1.03; P = .123*)
Median follow-up, mos 39.9 37.7
START: Overall Survival
353
757
188
429
Placebo
L-BLP25
410
829
285
617
127
301
108
255
88
204
59
128
33
73
18
33
4
8
0
0
Pts at Risk, n
Su
rviv
al (%
)
Butts CA, et al. ASCO 2013. Abstract 7500. Used with permission.
*2-sided, strata and multiplicity adjusted
Mos
L-BLP25
Placebo
100
90
80
70
60
50
40
30
20
10
0 0 6 12 18 24 30 36 42 48 54 60 66

Region
0.86 (0.67-1.11)
0.90 (0.74-1.09)
0.79 (0.58-1.09)
0.91 (0.71-1.17)
0.95 (0.73-1.22)
0.85 (0.65-1.11)
0.91 (0.75-1.10)
0.78 (0.64-0.96)
1.11 (0.86-1.43)
Favors L-BLP25
Stage IIIA (n = 487)
Stage IIIB (n = 752)
NA and Aus. (n = 321)
W. Europe (n = 475)
Rest of world (n = 443)
SD (n = 396)
Obj. response (n = 843)
Concurrent (n = 806)
Sequential (n = 433)
Stage
Response
to chemo/RT
Chemo/
RT type
Median OS, Mos
L-BLP25 vs Placebo
HR* (95% CI)
Favors Placebo *Not adjusted for strata.
Butts CA, et al. ASCO 2013. Abstract 7500. Used with permission.
START: OS Analyses by
Randomization Strata
27.6 vs 23.1
23.7 vs 20.9
34.1 vs 21.7
24.2 vs 22.3
21.8 vs 22.7
20.4 vs 17.8
27.8 vs 23.9
30.8 vs 20.6
19.4 vs 24.6
0.5 1.0 2.0

START: OS in Patients With
Concurrent Chemo/RT
L-BLP25 (n = 538)
Placebo (n = 268)
Median OS, mos 30.8 20.6
HR 0.78 (95% CI: 0.65-0.95; P = .016*)
227
499
118
295
Placebo
L-BLP25
268
538
186
412
73
205
62
176
54
147
40
89
26
51
16
24
4
7
0
0
Pts at Risk, n
Su
rviv
al (%
)
*2-sided, adjusted for strata
Mos
L-BLP25
Placebo
100
90
80
70
60
50
40
30
20
10
0 0 6 12 18 24 30 36 42 48 54 60 66
Butts CA, et al. ASCO 2013. Abstract 7500. Used with permission.

START: Safety
AE, % Tecemotide (n = 1024)
Placebo (n = 477)
Most frequent AEs (> 10% in tecemotide arm)
Cough 33.0 27.9
Dyspnea 23.2 23.5
Fatigue 19.2 21.4
Back pain 14.3 11.1
Nausea 13.7 8.2
Chest pain 13.2 9.4
Nasopharyngitis 12.5 9.2
Headache 12.1 11.3
Decreased appetite 10.6 9.2
Arthralgia 10.5 7.1
Influenzalike symptoms
• Any 38.2 33.1
• Grade 3/4 1.5 1.7
Pa
tie
nts
(%
)
Butts CA, et al. ASCO 2013. Abstract 7500. Used with permission.
100
90
80
70
60
50
40
30
20
10
0
91.6 90.6
33.4 35.8
29.6 31.7
4.5 7.3
Any AE Any
Grade
3/4 AE
Any
Serious
AE
Any AE
Leading
to Death
Tecemotide (n = 1024)
Placebo (n = 477)

Summary
• Study did not meet primary endpoint of significant improvement in OS with use of tecemotide maintenance
• Prespecified subgroup analysis identified significant 10.2-mo OS benefit with tecemotide in patients who received concurrent initial chemotherapy and radiotherapy
• Tecemotide therapy was well tolerated
– AE incidence similar to placebo



























#2658: Interim analysis of the Spanish Lung Cancer Group (SLCG) randomized phase II trial of thoracic radiotherapy (RT) concurrent with cisplatin (P) plus oral vinorelbine (OV) or etoposide (E) for unresectable locally advanced (LA) stage III non-small cell lung cancer (NSCLC). (GECP10/02).
Dolores Isla1, Ramon De Las Penas, Natividad Martinez-Banaclocha, Bartomeu Massuti, Maria Angeles Sala, Isabel Bover, Raquel Marse, Amelia Insa, Teresa Moran, Angel Artal, Pilar Diz, Jose Gomez-Codina, Ana Laura Ortega, Vanesa
Gutierrez, Jose Munoz, Melchor Alvarez De Mon, Carlos Camps, Ramon Garcia-Gomez, Jose M. Jurado, Santiago Ponce-Aix, Mariano Provencio

# 2658: Interim analysis of the Spanish Lung Cancer Group (SLCG) randomized phase II trial of thoracic radiotherapy (RT) concurrent with cisplatin (P) plus oral vinorelbine (OV) or etoposide (E) for unresectable locally advanced (LA) stage III non-small cell lung cancer (NSCLC). (GECP10/02). Dolores Isla
STUDY DESIGN
Multicentric randomized phase II trial Patients with non-resectable stage IIIA – IIIB NSCLC PS ECOG 0-1, Age ≤ 75 years, Weight loss < 5% / 3 m., Adequate lung function
Arm A: 2 cycles Induction CT: Vinorelbine Oral 80 mg/m2 (1st cycle 60 mg/m2) D1 D8 CDDP 80 mg/m2 D1 Every 3 weeks
2 cycles Concomitant CT-RT: Vinorelbine Oral 40 mg/m2 D1 D8 CDDP 80 mg/m2 D1
RT 66 Gy Every 3 weeks
Arm B: 2 cycles Concomitant CT-RT: Etoposide 50 mg/m2 D1 to D5
CDDP 50 mg/m2 D1 D8
RT 66 Gy Every 4 weeks
Thoracic RT: Standard 3D conformal RT by linear accelerator with >6 MV rays, Total dose: 66 Gy / 33 daily fractions / 2 Gy (5 dy/w)
Total sample size: 67 patients per arm Accrual start date: August 2011

CHARACTERISTIC ARM A
OVNR + CDDP N=34
ARM B
E + CDDP N=34
Median age, yr (range) 64 (45-75) 60 (43-71)
Gender, %: Male
Female
91.2
8,8
88.2
11.8
ECOG PS, %: 0
1
58.8
41.2
32.4
67.6
Smokers, %: Current
Never
Former
47.1
2.9
50
50
0
50
Histology, %:Squamous
Adenocarcinoma
Large cell
55.9
41.2
2.9
52.9
44.1
2.9
Stage, %: IIIA
IIIB
IV*
52.9
44.1
2.9
47.1
52.9
0
# 2658: Interim analysis of the Spanish Lung Cancer Group (SLCG) randomized phase II trial of thoracic radiotherapy (RT) concurrent with cisplatin (P) plus oral vinorelbine (OV) or etoposide (E) for unresectable locally advanced (LA) stage III non-small cell lung cancer (NSCLC). (GECP10/02). Dolores Isla
N of Participating Sites: 25 N of Patients Analized: 68 (total of 134)
PATIENT CHARACTERISTICS
* 1 inclusion failure, who did not receive study treatment but included in the ITT analysis.

RESPONSE * ARM A
OVNR + CDDP N=22
ARM B E + CDDP
N=24
CR 4.5 % 4.2 %
PR 63.7 % 50 %
OR (CR + PR) 68.2 % 54.2 %
SD 22.7 % 29.1 %
PD 9.1 % 16.7 %
RESPONSE RATE
# 2658: Interim analysis of the Spanish Lung Cancer Group (SLCG) randomized phase II trial of thoracic radiotherapy (RT) concurrent with cisplatin (P) plus oral vinorelbine (OV) or etoposide (E) for unresectable locally advanced (LA) stage III non-small cell lung cancer (NSCLC). (GECP10/02). Dolores Isla
* Evaluable population

HEMATOLOGICAL
TOXICITIES % of cycles
ARM A OVNR + CDDP
N = 98 cy
ARM B
E + CDDP
N = 56 cy
Anemia 0 3.57
Neutropenia 6.12 12.50
Febrile neutropenia 3.06 1.79
Leucopenia 2.04 8.93
Thrombocytopenia 0 5.36
NON-
HEMATOLOGICAL
TOXICITIES % of cycles
ARM A OVNR +
CDDP
N = 98 cy
ARM B E + CDDP
N = 56 cy
Asthenia/fatigue 1.02 1.79
Diarrhoea 1.02 0
Esophagitis 0 8.93
Infection 1.02 7.14
Mucositis 1.02 1.79
Alopecia (grades 1/2) 6.12 37.5
# 2658: Interim analysis of the Spanish Lung Cancer Group (SLCG) randomized phase II trial of thoracic radiotherapy (RT) concurrent with cisplatin (P) plus oral vinorelbine (OV) or etoposide (E) for unresectable locally advanced (LA) stage III non-small cell lung cancer (NSCLC). (GECP10/02). Dolores Isla
TOXICITY Grade ¾

Safety Data from a Phase II Study of Pemetrexed (PEM) and Cisplatin (CIS) with Concurrent Thoracic Radiation after PEM+CIS Induction in
Patients with Unresectable Locally Advanced (LA) Non-Squamous Non-Small Cell Lung Cancer (NS-NSCLC)
P. Garrido1, M. Serke2, S. Novello3, P. Giraud4, C. Visseren-Grul5, S. Ameryckx6, V. Soldatenkova7,
N. Chouaki8, W. Engel-Riedel9
1University Hospital Ramon Y Cajal, Madrid, Spain; 2Hemer Lung Clinic, Hemer, Germany; 3S. Luigi Hospital, University of Turin, Orbassano, Italy; 4Georges Pompidou European Hospital, Paris, France; 5Medical Oncology, Eli Lilly and Company, Houten, The
Netherlands; 6Global Clinical Trial Management, Lilly S.A. Eli Lilly Benelux N.V., Brussels, Belgium; 7European Statistics, Oncology, Lilly Deutschland GmbH, Bad Homburg, Germany; 8Medical Oncology, Lilly France, Neuilly sur Seine, France; 9Lung Clinic Merheim, Hospital
of Cologne, Cologne, Germany

Background
• Concurrent chemo- and radiotherapy (CT+RT) is standard of care for most patients with locally advanced unresectable NSCLC, but no specific CT regimen is recommended1,2
• PEM synergizes with ionizing radiation and CIS in preclinical models3,4
• PEM+CIS doublets showed efficacy and favourable toxicity profiles in Phase I/II studies of locally advanced NSCLC when combined with thoracic RT5,6
• Concurrent CT+RT preceded by induction has been tested in Phase III, using a CARBO-based regimen1,7
1Vansteenkiste et al., Ann Oncol 2013 [epub]; 2Auperin et al., J Clin Oncol 2010;28:2181-90; 3Wagner and Yang, Curr Drug Targets 2010;11:67-73 4 Bischof et al., Int J Radiat Oncol Biol Phys 2002;52:1381-88 5 Brade et al., Int J Radiat Oncol Biol Phys 2011;79:1395-401 6 Gadgeel et al., J Thorac Oncol 2011;6:927-33 7 Vokes et al., J Clin Oncol 2007;25:1698-704

Objectives
• Primary objective: To assess the antitumor activity of PEM+CIS as induction, followed by PEM+CIS with concurrent thoracic RT, as measured by 1-year progression-free survival (PFS) rate
• Secondary objectives:
– Objective tumor response rate (RR)
– Overall survival (OS)
– Safety and tolerability

Study Design
1American Joint Committee on Cancer TNM Staging System for Lung Cancer, 6th edition, 2002
2Response Evaluation Criteria in Solid Tumors (RECIST) guidelines, version 1.0; Therasse et al., J Natl Cancer Inst 2000;92:205-16.
All patients received folic acid, vitamin B12 and dexamethasone as per PEM label
Treatment Period
Induction CT (2 cycles) Concurrent CT (2 cycles) + RT
500 mg/m2 pemetrexed +
75 mg/m2 cisplatin, d1, q21d
Concurrent CT + RT started if:
• CR, PR, SD
• ECOG PS 0/1
Patients enrolled if:
• Non-squamous NSCLC
• Stage IIIA/IIIB (AJCC Version 6)1
• ECOG PS 0/1
500 mg/m2 pemetrexed +
75 mg/m2 cisplatin, d1, q21d
3D conformal RT:
Total dose 66 Gy
33 fractions of 2 Gy
FU
≥ 2 years
follow-up
2

Summary of CT and RT Exposure
Cycles received, n (%) All patients (N = 90)
Completed 2 cycles of induction CT 85 (94.4)
Started concurrent CT+RT 75 (83.3)
Completed 4 cycles of CT 72 (80.0)a
a 64/72 patients also received ≥60 Gy of RT („completed treatment“)
RT dose received, n (%) All patients (N = 90)
Started concurrent CT+RT 75 (83.3)
Received full dose (66 Gy) 65 (72.2)
Received 60 to <66 Gy 4 (4.4)
Received <60 Gyb 6 (6.7)
b Range 18 – 52 Gy/9 – 26 fractions

Time (months)
0 6 12 18 24 30
PF
S P
rob
ab
ilit
y
0.0
0.2
0.4
0.6
0.8
1.0
Progression free survival

Proximity of Disease Progression to Radiation Field
All patients (N = 90) n (%)
With documented disease progression 53 (58.9)
With PD and not eligible to receive RT 12 (13.3)
Documented PD and started CT+RT 41 (45.6)
Local disease progression 19 (21.1)
Within radiation field 14 (15.6)
Outside of radiation field, within thorax 5 (5.6)
Distant metastases 22 (24.4)

Tumor Response (RECIST 1.0)
All patients (N = 90)
Best overall response n (%)
Complete response (CR) 7 (7.8)a
Partial response (PR) 46 (51.1)
Response rate (CR+PR) 53 (58.9) 95% CI: 48.0, 69.2
Stable disease (SD) 17 (18.9)
Disease control rate (CR+PR+SD) 70 (77.8) 95% CI: 67.8, 85.9
Progressive disease (PD) 12 (13.3)
Not evaluableb/not done 7b/1 (7.8/1.1)
a 3 patients after CT+RT, 4 patients after CT+RT + surgery b 7 patients who discontinued study treatment before starting the concurrent CT+RT phase due to reasons other than
PD were considered as not evaluable for best overall response.
RECIST 1.0: Therasse et al., J Natl Cancer Inst 2000;92:205-16

Safety Data – Overview
All patients (N = 90) n (%) with event
Any treatment-emergent adverse event (TEAE) 85 (94.4)
Grade 3/4 TEAEs 38 (42.2)
Related to study treatment 33 (36.7)
Serious TEAEs 23 (25.6)
Related to study treatment 17 (18.9)
Death due to toxicity 1 (1.1)a
Adverse events leading to discontinuation 6 (6.7)
Related to study treatment 4 (4.4)b
a Death due to enteritis, during concurrent CT+RT, Cycle 4 b 1 patient had renal failure, 1 patient had hypoacusis, 2 patients had radiation esophagitis
Analysis of adverse events according to NCI-CTCAE, Version 3.0 .
Available at: http://ctep.cancer.gov/protocolDevelopment/electronic_applications/docs/ctcaev3.pdf

Grade 3/4 Toxicities (CTCAE)
Number (%) of patients with G3/4 CTCAEs
During Induction CT
N = 90
During conc. CT+RT N = 75
During complete treatment period
N = 90
Hematologic
Neutropenia 2 (2.2) 8 (10.7) 8 (8.9)
Leukopenia 0 7 (9.3) 7 (7.8)
Thrombocytopenia 0 2 (2.7) 2 (2.2)
Anemia 0 1 (1.3) 1 (1.1)
Non-hematologic toxicities a,b
Esophagitis/dysphagia 0 9 (12.0) 9 (10.0)
Mucositis 0 1 (1.3) 1 (1.1)
Acute pneumonitis 1 (1.1) 1 (1.3) 2 (2.2)
a Selected based on clinical relevance for combined CT+RT b Only 1 G4 esophagitis, all other events reported in Table were G3

Conclusions
In this study of PEM+CIS induction, followed by concurrent full-dose PEM+CIS plus RT in patients with locally advanced NS-NSCLC:
• PFS (1-year rate 51.3%) was in the same range as previously observed with other CIS-based induction CT followed by concurrent CT+RT1,2
• The overall response rate was 58.9% (disease control rate 77.8%)
• Delivery of full dose PEM+CIS CT+RT was feasible, with 71% of patients completing treatment
• Grade 3/4 toxicities ≥10% during concurrent CT+RT included esophagitis (12%) and neutropenia (11%), which are considered acceptable for locally advanced NSCLC
1 Descourt et al., J Thorac Oncol 2011;6:351-57 2Fournel et al., J Clin Oncol 2006; 24(June 20 Suppl):7048


Comentarios a futuro: ¿Denver 2015?
• Es necesario realizar estudios en subgrupos específicos de los estadios IIIA-IIIB
• Son necesarios factores predictivos de individualización terapéutica
• Son necesarios estudios en las poblaciones mayoritarias (comorbilidad, edad)
• Es necesario incluir en objetivos de los estudios toxicidad y valoración subjetiva

Albert Camus (1913-1960)
• Adquirimos la costumbre de vivir antes que la de pensar". (El mito de Sísifo).
• “Lo que más distingue al hombre del animal es la imaginación”. (Carnets 2)
A. Camus Obras Completas Alianza Editorial. Madrid 1996